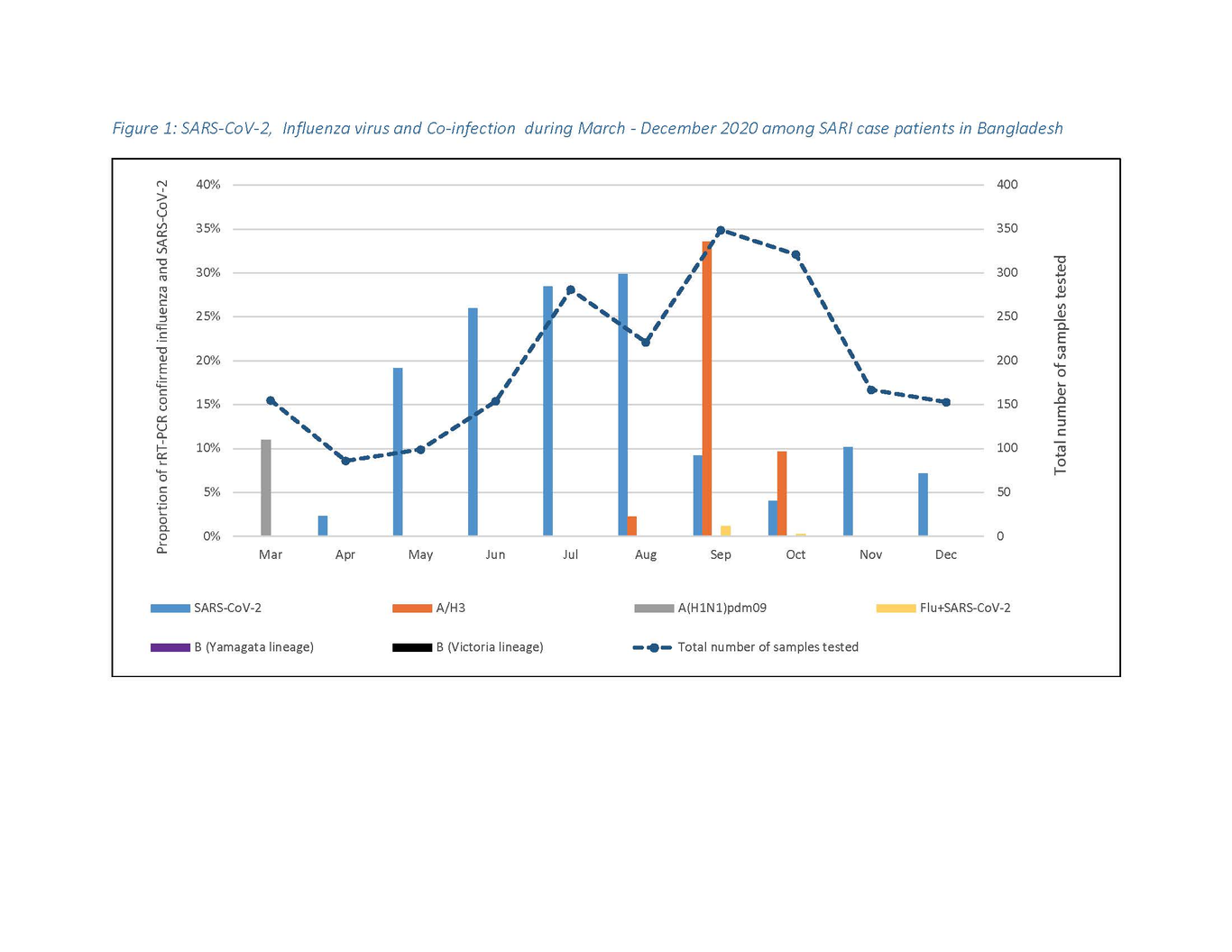
Background: Recent evidences reported that co-infection with SARS-CoV-2 and Influenza virus is common. We explored hospital-based influenza surveillance (HBIS) data during the COVID-19 pandemic. Methods: We analyzed data from March to December 2020 among patients admitted with severe acute respiratory infections (SARI) defined as subjective or measured fever of ≥ 38 C° and cough with onset within the last ten days. Physicians recorded patients’ demographic, clinical, and laboratory information and obtained nasopharyngeal and oropharyngeal swabs to test for influenza virus and SARS-CoV-2 by rRT-PCR. Results: We enrolled 1,986 SARI case-patients with median age of 28 years (IQR: 1.2 53 years), and 67.6% were male. Among SARI case-patients, 285 (14.3%) were infected with SARS-CoV-2 and 175 (8.8%) infected with influenza virus. Only five (0.3%) SARI patients were co-infected with SARS-CoV-2 and influenza virus. Difficulty breathing (83% vs. 77%, p=0.024) and sore throat (26% vs. 17%, p<0.001) were more likely to be present in SARS-CoV-2-infected SARI patients. SARI case-patients with diabetes and hypertension were more likely (14% vs. 6%, p<0.001 and 27% vs. 12%, p<0.001 respectively) to be infected with SARS-CoV-2 virus than those without co-morbidities. Influenza virus remained undetectable during the first 14 weeks of the 20 weeks (May to September) of peak influenzacirculation period in Bangladesh. Conclusions: Our findings suggest that co-infection with SARS-CoV-2 and influenza virus was not very common together with nonappearance of the influenza virus during most of the peak influenza period in Bangladesh during COVID-19 pandemic. Future studies are warranted for further exploration.