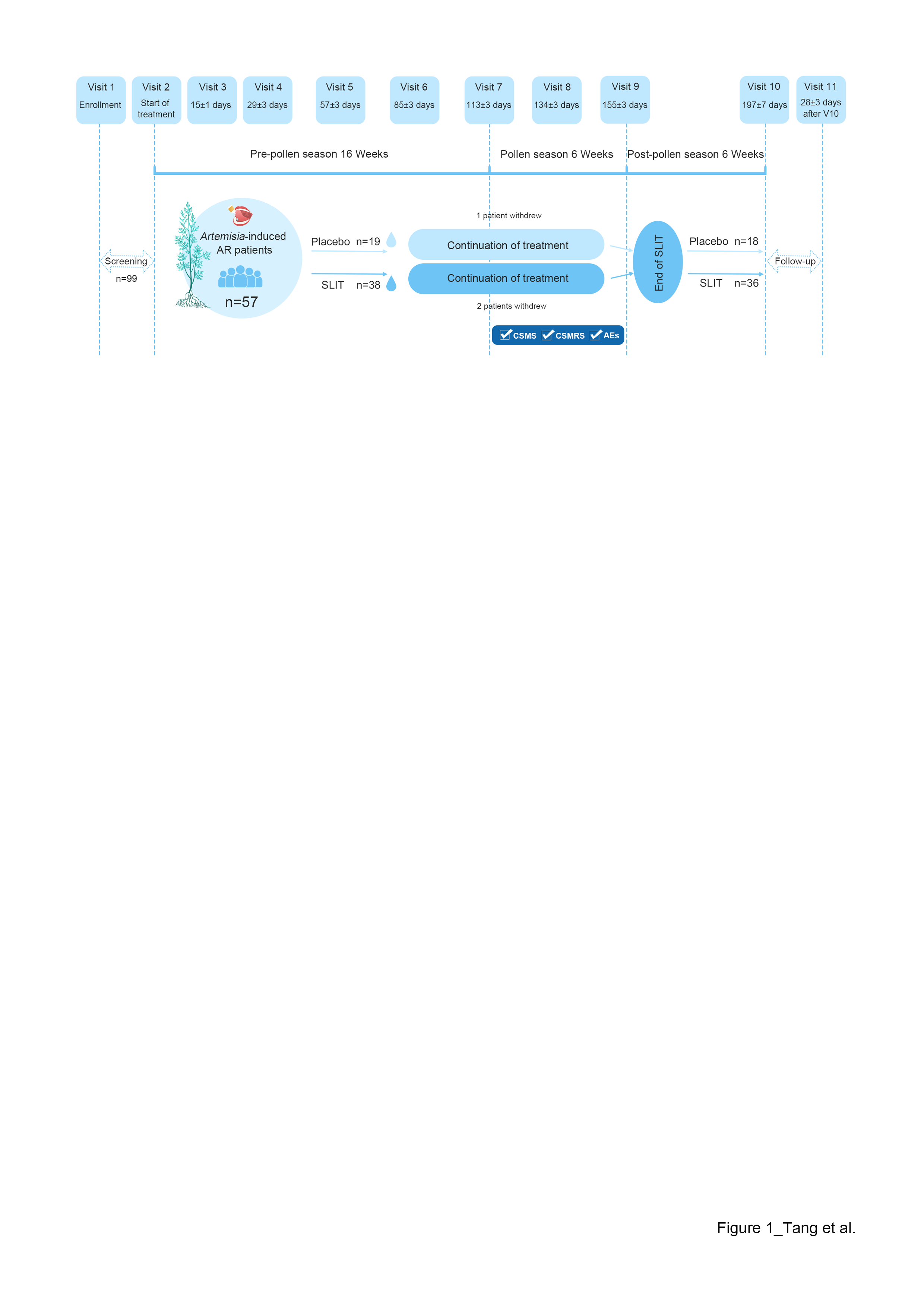
Artemisia annua sublingual immunotherapy in children with seasonal allergic rhinitis To the Editor,Artemisia pollen is the main aeroallergen of seasonal allergic rhinitis (SAR) in summer and autumn.1,2Artemisia annua Allergens Sublingual Immunotherapy (SLIT) Drops (Zhejiang Wolwo Bio-Pharmaceutical Co., Ltd., Zhejiang, China, National Drug Approval No.: S20210001) is the only standardized SLIT preparation approved in China for treatingArtemisia-induced allergic rhinitis with or without conjunctivitis (AC).3 In this study, we aimed to evaluate the safety and efficacy of A. annua- SLIT in children with SARs.Pediatric patients with at least a two-year clinical history ofArtemisia pollen-induced SAR with or without AC from Inner Mongolia were included in this randomized, double-blind, placebo-controlled, single-center clinical trial and randomized to receive A. annua -SLIT or placebo at a 2:1 ratio for approximately 28 weeks. The combined score of medication and rhinitis symptoms (CSMS; primary endpoint) and combined score of medication and rhinoconjunctivitis symptoms (CSMRS; secondary endpoint) were recorded to evaluate efficacy; adverse events (AEs) were reported to assess safety.Fifty-seven eligible patients aged 4–18 years were randomized into the SLIT (n=38) and placebo (n=19) groups (Figure 1). Finally, 54 patients (SLIT group: n=36; placebo group: n=18) completed the study with 3 patients withdrew by themselves. No significant differences were observed between the groups in terms of sex, age, atopic status, comorbidity of other allergic diseases, and CSMS and CSMRS scores in the previous pollen season (P >0.05, Table S1).The 2019 pollen season in Inner Mongolia was from 20th July to 7th September (50 days; Figure 2A). The temporal variation of daily CSMRS in both groups showed a similar trend of positive correlation with pollen concentration throughout the pollen season (SLIT group: r=0.66, 95% CI: 0.53–0.76; placebo group: r=0.68, 95% CI: 0.56–0.77). The SLIT group showed significant improvements in CSMS (1.55±0.81 vs. 1.97±0.73) and CSMRS (1.46±0.75 vs. 1.88±0.75) compared with the placebo group (P <0.05, Figure 2B–C). Fifty-three (98.1%) patients experienced AEs [35, SLIT group; 18, placebo group] (Table S2). All AEs were mild or moderate and resolved without any action or by adjusting the dose of the study drug. There were no significant differences in the incidence and severity of AEs between the groups (P >0.05). Epinephrine use was not reported, and no patients withdrew from the trial because of AEs. Furthermore, 94.4% and 100% of patients in the SLIT and placebo groups, respectively, experienced treatment-related AEs (TRAEs), which frequently occurred in the nose, eyes, throat, and tongue in both groups (P >0.05, Figure 2D). The common TRAEs in children with SLIT are shown in Figure 2E. Most TRAEs in the SLIT group were mild, similar to those in the placebo group.To our knowledge, this is the first study to report the efficacy and safety of A. annua -SLIT in a Chinese pediatric population. Our results showed a consistent trend of clinical efficacy improvements withA. annua -SLIT in children similar to those in adults.4 Recently, a cumulative AE incidence of 93.0% was reported with ragweed SLIT in children and adolescents, with no serious AEs.5 The incidence of AEs in our study were comparable to those in the previous study. Lou et al. found that the most common TRAEs in adults with A. annua -SLIT were mild or moderate.4,6 Our results showed a safety profile similar to that in adults. No new safety signals emerged, and no throat irritation was observed in adults.In conclusion, 28-week A. annua -SLIT treatment was effective and safe for children with SAR, with no major safety concerns. Investigating the benefits of A. annua -SLIT in children will not only expand its application for treatment but also provide the basis for intervention in the early phase of SAR.