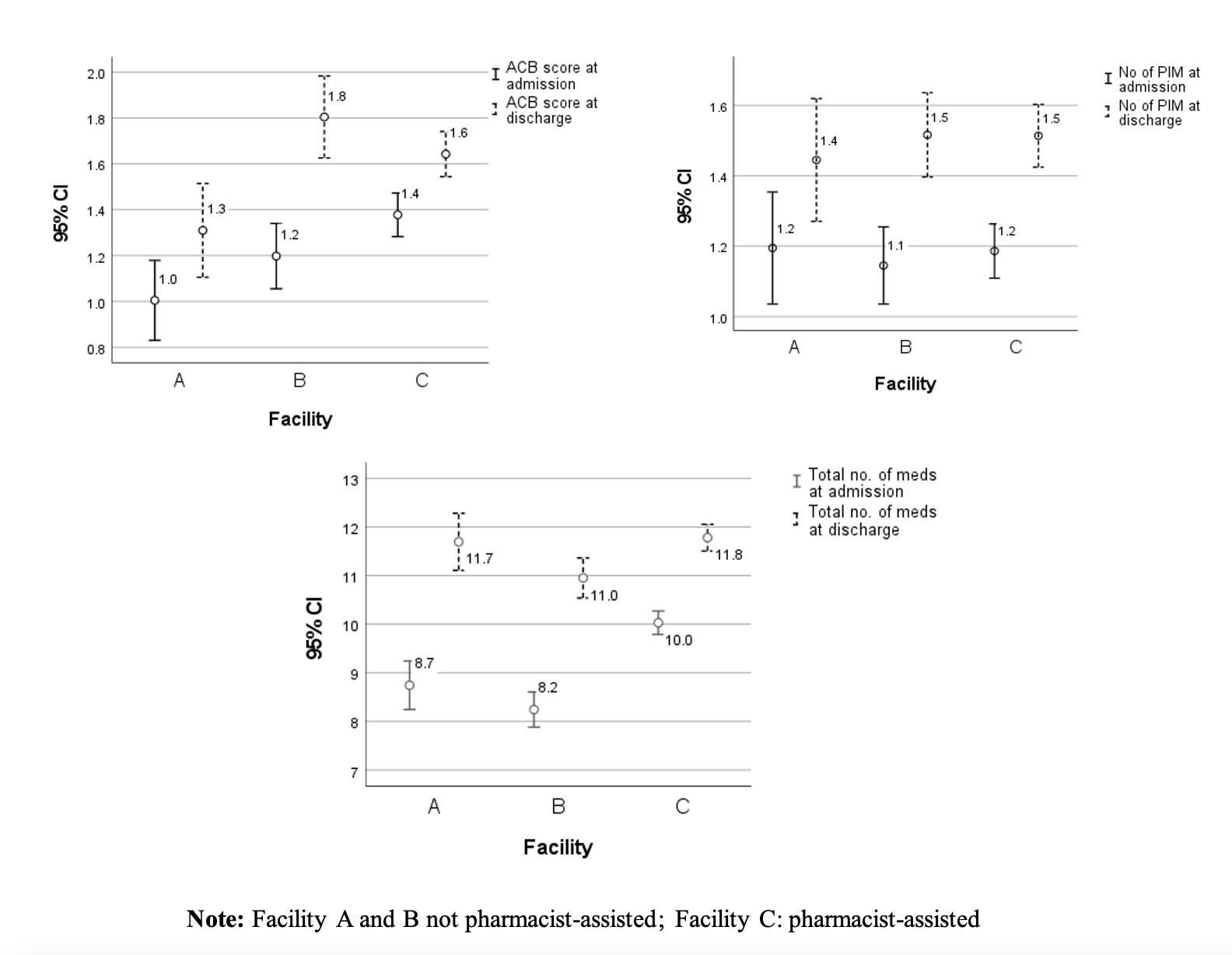
Aim. To investigate the impact of pharmacists’ presence in long-term care facilities (LTCFs) on medication usage. Methods. The study followed a retrospective cohort design, with a sample of patients aged ≥ 65 years old admitted to 3 LTCFs over 30 months. Data on age, gender, type of stay, presence/absence of pharmacist and medication at admission and discharge were obtained for study patients. Variations in the number of medicines (NoM), anticholinergic burden (ACB), and potentially inappropriate medication (PIMs), at admission and discharge, were assessed as outcome variables. Anticholinergic burden and PIMs were identified using the Anticholinergic Cognitive Burden scale and the EU(7)-PIM List, respectively. One-sample t-tests were applied to compare outcome variables’ mean values at admission and discharge. A 4-way ANOVA was employed to test the association between background and outcome variables. Partial Eta squared (η2) was used to measure the effect size. Results. The 3 LTCFs assisted 1643 patients during the study period, of which 1366 were included in data analysis. Only one LTCF had pharmacy services. All outcome variables showed a statistically significant increase at discharge compared with admission. Pharmacist’s presence was statistically significant at improving the NoM (p<0.001) and ACB score (p<0.001), while no statistically significant value was reached on PIMs (p = 0.642). Small effect size values were reached for pharmacist impact on the NoM and ACB score (η2 = 0.021, η2 = 0.011, respectively). Conclusion. The present findings suggest that pharmacists’ presence positively impacts the use of medications implicated in adverse health outcomes in LTC patients.