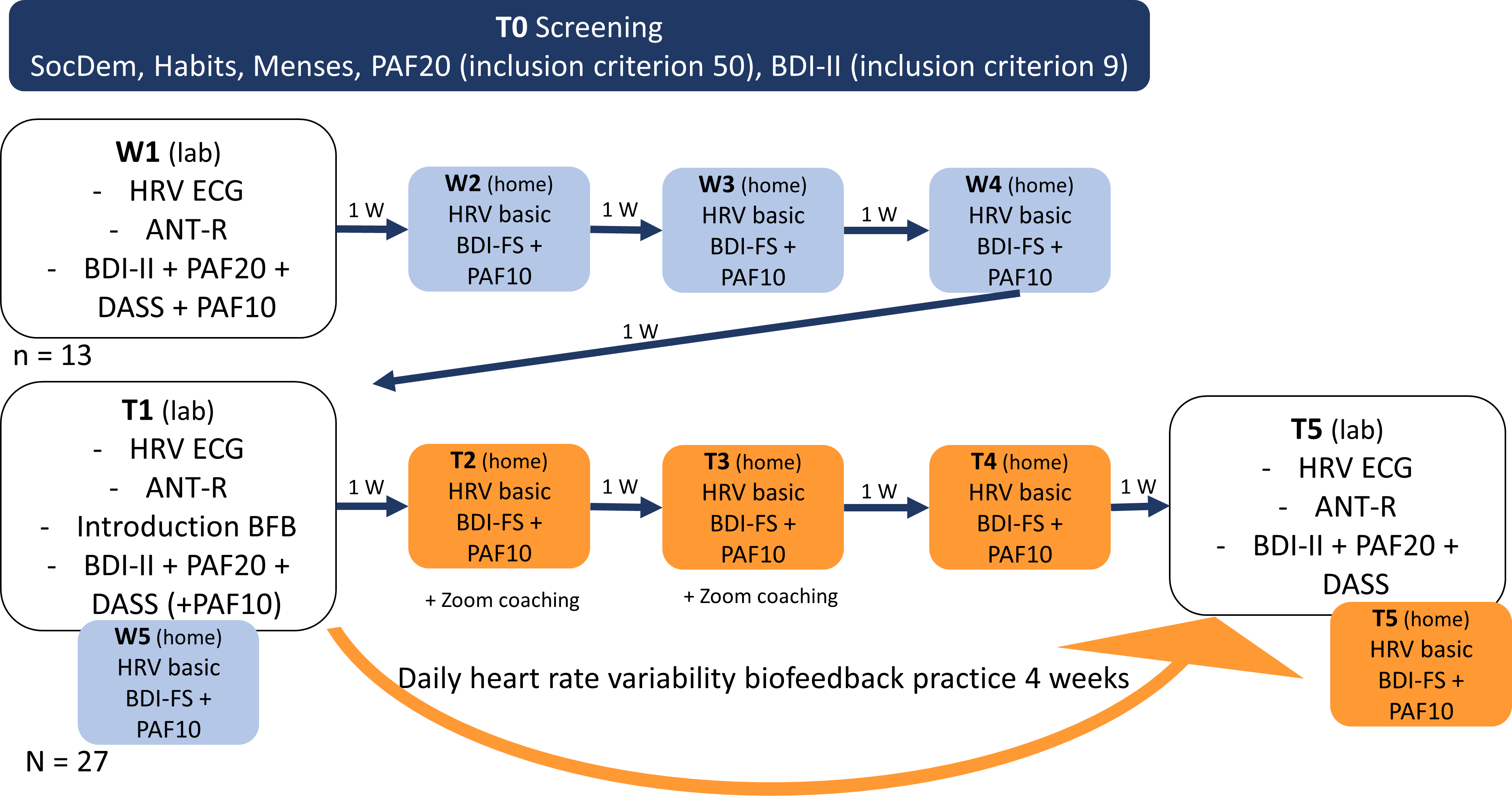
Berenike Lisa Blaser1*, Mathias Weymar1,2, & Julia Wendt11 University of Potsdam, Department of Biological Psychology and Affective Science, Faculty of Human Sciences, Karl-Liebknecht Strasse 24/25, 14476 Potsdam, Germany2Faculty of Health Sciences Brandenburg, University of Potsdam, Potsdam, Germany * Correspondence:Berenike Lisa BlaserUniversity of PotsdamKarl-Liebknecht Strasse 24/2514476 Potsdam, Germany Email: [email protected] Running head: Smartphone-based Heart Rate Variability Biofeedback for PMS Keywords: smartphone photoplethysmography, mHealth, heart rate variability, biofeedback, vagal tone, premenstrual syndrome, premenstrual symptoms, menstrual cycle, stress, depression, attentional control AbstractIntroductionHeart rate variability biofeedback (HRVB) is a well-studied intervention known for its positive effects on emotional, cognitive, and physiological well-being, including relief from depressive symptoms. However, its practical use is hampered by high costs and a lack of trained professionals. Smartphone-based HRVB, which eliminates the need for external devices, offers a promising alternative, albeit with limited research. Additionally, premenstrual symptoms are highly prevalent among menstruating individuals, and there is a need for low-cost, accessible interventions with minimal side effects. With this pilot study, we aim test, for the first time, the influence of smartphone-based HRVB on depressive and premenstrual symptoms, as well as anxiety/stress symptoms and attentional control.MethodsTwenty-seven participants with above-average premenstrual or depressive symptoms underwent a 4-week photoplethysmography smartphone-based HRVB intervention using a waitlist-control design. Laboratory sessions were conducted before and after the intervention, spaced exactly 4 weeks apart. Assessments included resting vagally mediated heart rate variability (vmHRV), attentional control via the revised attention network test (ANT-R), depressive symptoms assessed with the BDI-II questionnaire, and stress/anxiety symptoms measured using the DASS questionnaire. Premenstrual symptomatology was recorded through the PAF questionnaire if applicable. Data analysis employed linear mixed models.ResultsWe observed improvements in premenstrual, depressive, and anxiety/stress symptoms, as well as the Executive Functioning Score of the ANT-R during the intervention period but not during the waitlist phase. However, we did not find significant changes in vmHRV or the Orienting Score of the ANT-R.DiscussionThese findings are promising, both in terms of the effectiveness of smartphone-based HRVB and its potential to alleviate premenstrual symptoms. Nevertheless, to provide a solid recommendation regarding the use of HRVB for improving premenstrual symptoms, further research with a larger sample size is needed to replicate these effects. 1 IntroductionHeart rate variability biofeedback (HRVB) is a well-researched intervention that has demonstrated effectiveness in a wide range of areas (Lehrer et al., 2020), including relieving anxiety and stress (Goessl et al., 2017), ameliorating depression (Pizzoli et al., 2021), improving sleep (Stein & Pu, 2012), alleviating asthma symptoms (Lehrer et al., 2004), and even enhancing sports performance (Jiménez Morgan & Molina Mora, 2017). However, despite its potential, this user-friendly method has seen limited practical implementation. This can be attributed, in part, to the high costs associated with necessary stationary and mobile electrocardiography (ECG) devices, as well as the required training and expertise of staff members entrusted with its administration, which further strains healthcare systems. Encouragingly, smartphone apps capable of assessing heart rate through the device's camera, without additional equipment, are promising to yield similar results (Yuda et al., 2020). Nevertheless, empirical validation of smartphone-based HRVB applications remains limited. This study aims to validate the effectiveness of an HRVB intervention applied through smartphones, specifically targeting the alleviation of depressive symptoms, a well-documented outcome of conventional HRVB. Additionally, we explore a novel application of HRVB for premenstrual symptoms.HRVB is a method in which vagally mediated heart rate variability (vmHRV), an indicator of parasympathetic activity (Laborde et al., 2023; Penttilä et al., 2001), is systematically increased through slow, controlled breathing and visual feedback of heart rate oscillations. The primary driving mechanism involves slow-paced breathing at 0.1 Hz or an individual resonance frequency (Laborde, Allen, Borges, Iskra, et al., 2022). It is believed to exert its various beneficial effects through bottom-up modulation of a neural network described by Thayer and Lane (2000) in their neurovisceral integration model. This model delineates a network of interconnected structures known as the central autonomic network (CAN), responsible for integrating information and regulating appropriate responses. At the core of this regulatory network, Thayer and Lane (2009) propose an inhibitory connectivity between the medial prefrontal cortex (mPFC) and the amygdala. The stronger this connectivity, the greater an individual's capacity to downregulate a presumed default stress response and deliver a precise and personalized reaction to internal and environmental demands. VmHRV is considered both a peripheral index for this capacity and a reciprocal element within this network (Thayer et al., 2009). This theory is grounded in a substantial body of evidence linking low vmHRV to psychopathology (Heiss et al., 2021) and reduced performance in cognitive self-control tasks (Holzman & Bridgett, 2017; Zahn et al., 2016). When practiced over several weeks, HRVB enhances the capacity of the CAN through coherence phenomena involving the synchronization of breathing rate, blood pressure, and heart rate oscillations (Sevoz-Couche & Laborde, 2022). These phenomena contribute to several bottom-up routes. The most crucial of these routes involve input into the CAN through baroreceptors via the nucleus of the solitary tract, stretch receptors in the lungs, and a vagal afferent pathway (Lehrer & Gevirtz, 2014; Noble & Hochman, 2019; Sevoz-Couche & Laborde, 2022).HRVB interventions have demonstrated the potential to improve various affective and cognitive outcomes associated with CAN capacity, including depression (Pizzoli et al., 2021) and anxiety (Goessl et al., 2017). Our study aims to expand these effects in the context of a smartphone-based intervention. While vmHRV is reliably associated with cognitive outcomes, particularly executive functions, the impact of HRVB on these variables is less clear (Tinello et al., 2022). In a systematic review, Tinello et al. (2022) found that existing effects are primarily observed in the domain of attentional control and are often found in patient populations or individuals experiencing high levels of stress. Given that attention is strongly linked to vmHRV, we also investigate the effect of HRVB on attentional control using the revised Attention Network Test (ANT-R, Blaser et al., 2023a; Fan et al., 2009).Expanding on these replications, we further investigate HRVBs impact on premenstrual syndrome (PMS), a highly prevalent condition characterized by a diverse collection of psychological and physiological symptoms. These symptoms typically manifest in individuals with active menstrual cycles during the week leading up to menstruation and tend to subside shortly after. As many as 90% of menstruating individuals regularly encounter at least one symptom of PMS (Tschudin et al., 2010). Commonly reported symptoms encompass heightened stress reactivity, anxiety, depressive mood, breast tenderness, and abdominal pain (Allen et al., 1991).As a component of the gender data gap, premenstrual syndrome (PMS) remains significantly under-researched (Zehravi et al., 2023). Even today, treatment options remain limited, primarily centered on addressing specific psychological or physiological symptoms through hormonal cycle suppression or antidepressant medication in both clinical practice and research (Ryu & Kim, 2015). Both of these approaches are associated with substantial adverse side effects (Price et al., 2009; Robinson et al., 2004; Skovlund et al., 2016).Premenstrual symptoms have been linked to cyclic fluctuations in vagally mediated heart rate variability (vmHRV) (Schmalenberger et al., 2019). Individuals who experience more severe symptoms tend to exhibit a pronounced reduction in vmHRV during the luteal phase of their menstrual cycle, coinciding with the experience of these symptoms (Matsumoto et al., 2007). Matsumoto et al. (2007) have suggested a potential causal relationship in this regard. One possible explanation for this phenomenon lies in a metabolite of progesterone, one of the main fluctuating gonadal steroids during the menstrual cycle. Sundström-Poromaa et al. (2003) have identified this metabolite, namely Allopregnanolone (ALLO), an allosteric Gamma-Aminobutyric Acid (GABA) receptor modulator as a likely cause of the experience of premenstrual symptoms (Hantsoo & Epperson, 2020). As ALLO operates on the GABAergic system, the proposed CAN in the neurovisceral integration theory (Thayer & Lane, 2000, 2009) might also be affected. In this theory, successful adaptation relies on inhibitory connectivity between the mPFC and the amygdala. The strength of these connections, which are part of the central nervous system's inhibitory GABAergic network, are influenced by GABA levels in the mPFC (Delli Pizzi et al., 2017). Compromised inhibition in this circuit due to ALLO withdrawal and/or maladaptive ALLO responses may lead to a compromised self-regulatory capacity of the organism on both affective and physiological levels, as observed in PMS.Following this line of reasoning, HRVB is a promising candidate to counteract some of these effects through two mechanisms. Firstly, the most pronounced effects of HRVB are observed in stress management (Goessl et al., 2017). If stress throughout the cycle causes irregularities in the ALLO system during the premenstrual phase, reducing stress throughout the cycle may prevent some of the symptom development. Existing evidence already suggests that various relaxation techniques can positively impact PMS (Jose et al., 2022). Secondly, HRVB is assumed to increase the inhibitory capacity of the mPFC over the amygdala and, as a result, enhance the inhibition of the default stress response (Schumann et al., 2021). Although GABAergic transmission may be compromised during the premenstrual phase, boosting the baseline inhibitory strength between these two brain structures could raise inhibition levels. This might make it less likely for a sudden drop to cross the threshold to trigger symptoms that cause significant distress.Initial studies have already provided evidence of the effectiveness of HRVB for mental health outcomes when administered through smartphones. Previous studies that utilized smartphone-based HRVB interventions to improve outcomes like depressive or anxiety symptoms, however, have typically relied on external devices connected to the smartphone via Bluetooth. These devices include wearable ECG-measuring breast straps (Chung et al., 2021; Herhaus et al., 2022; Lin, 2018; Schumann et al., 2022; Schumann et al., 2021) or earlobe-clip pulse measuring devices (Economides et al., 2020; Minen et al., 2021; Schuman et al., 2023). Acquiring a wearable device presents a significant obstacle for potential HRVB users. Smartphone cameras can now measure heart rate when the user places a finger on the camera. An application activates the camera flash and analyzes the red-to-green ratio in the image at high frequency, generating pulse curves. This process is known as photoplethysmography (PPG) and closely resembles the process behind the optical sensors that emit infrared or green light in commonly used pulse measurement devices. Yuda et al. (2020) suggest that the heart rate variability indicator used in smartphone apps, which they term 'pulse rate variability' as measured through PPG, may contain distinct information compared to its ECG-measured counterpart. Nevertheless, recent research has demonstrated very high correlations between HRV parameters measured through ECG and PPG of over .9 (van Dijk et al., 2023), even though the reliability is somewhat dependent on sampling rate of the device (Guede-Fernández et al., 2020). Moreover, the associations with mental health outcomes are also evident when assessing vmHRV via PPG using the smartphone camera (Liu et al., 2020). This supports the use of PPG as a foundation for HRVB.In this study, we investigated the novel application of a 4-week smartphone-based HRVB intervention using PPG via smartphone camera instead of an external device for alleviating depressive and premenstrual symptoms. Our sample comprised young adults who either exhibited above-average PMS or depressive symptoms. Additionally, we examined the impact of the intervention on various other outcomes, including anxiety and stress symptoms, attentional control, and vmHRV.2 Methods2.1 ParticipantsA G*Power analysis revealed that a sample size of 40 was necessary to detect an effect size of .4, based on a meta-analytic effect of HRVBFB on depressive symptoms reported by Pizzoli et al. (2021), with a power of .8 and a one-tailed alpha error probability of .05. However, due to recruitment difficulties and resourcing issues by the company providing the app during the extended recruitment period, we were unable to reach our target of 40 participants.Twenty-nine participants were recruited from the student population of the University of Potsdam for this study. Recruitment was carried out via the online recruiting platform for study participants of the cognitive sciences (Sona Systems, https://www.sona-systems.com) of University Potsdam as well as via flyers on campus and advertisement in university mailing lists. Inclusion criteria required participants to have either above-average premenstrual symptomatology (short version Premenstrual Assessment Form, PAF20 ≥ 50), depressive symptoms that indicate at least minimal depression (Beck’s Depression Inventory, BDI-II ≥ 9), or both. Participants who exceeded a BDI-II score of 14 received a consultation with a clinical psychologist to discuss possible necessary treatment prior to study participation.Exclusion criteria included factors proposed by Laborde et al. (2017) such as pregnancy, heart rate-altering chronic diseases or medication. We additionally excluded competitive athletes to avoid ceiling effects, since this population has systematically increased vmHRV (Da Silva et al., 2015). Participants currently in any treatment or planning significant lifestyle changes during the period of study participation were also excluded. In addition, participants were required to be at least 18 years of age.All participants provided informed consent prior to their inclusion for a study protocol approved by the ethics committee of the University of Potsdam (No. 30/2022). Participants who met the inclusion criteria were eligible for study participation and received either course credits or monetary compensation.2.2 ProcedureThe study protocol was preregistered on Open Science Framework (osf.io/68fzq). The study procedure began with an online screening questionnaire to determine eligibility based on inclusion and exclusion criteria, as well as to assess sociodemographic factors such as age, gender, study program, and BMI. Participants were also required to provide information about their menstrual cycle to ensure that the appropriate questionnaires were administered. Additionally, participants were asked to provide their email address for communication throughout the study.All eligible participants took part in a 4-week biofeedback intervention during which they practiced smartphone-based HRVB for at least 5 minutes every day. After the first and second week, participants additionally received an online coaching session to improve their technique and address any technical or other difficulty they encountered.Before and after the 4-week intervention, participants completed laboratory sessions that were scheduled at the same time, exactly 4 weeks apart (T1 and T5). During these sessions, various measures were collected, including vagally mediated heart rate variability by ECG, attentional control using the reaction time paradigm ANT-R (Fan et al., 2009), and self-reported symptoms of depression, premenstrual syndrome (PMS), and anxiety/stress via questionnaires.To ensure balanced allocation of participants to the waitlist group, half of the participants within each group of inclusion criteria (depression, PMS, or both) were pseudo-randomly assigned to the waitlist group. The waitlist group additionally completed a laboratory session four weeks prior to study inclusion, during which the same parameters were assessed (W1).Throughout the study, participants completed short versions of the depressive and premenstrual symptom questionnaires and underwent a photoplethysmography based HRV measurement at home using the biofeedback app, each week on the same day and at the same time that they chose (W2-W4 and T2-T4). Participants received automated email reminders and a link to the respective questionnaire to ensure compliance. The results of these measurements are not analysed and reported in this report. Figure 1 provides an overview of the study procedure.All participants received an introduction to smartphone-based HRVB during T1. The waitlist group received a tutorial on conducting vmHRV measurements at home with the app during W1, while the intervention-only group received this tutorial during T1.Since PMS occurs only once during each menstrual cycle, and cycle lengths can vary significantly both between and within individuals, we included a follow-up measurement of the online questionnaire 4 weeks after T5. If a participant reported no new menstruation onset during the last two weeks of the intervention, indicating no new premenstrual phase, we used the PMS values reported in the follow-up measurement as the post-intervention values, describing the next premenstrual phase after completing the intervention. Figure 1. Study procedure