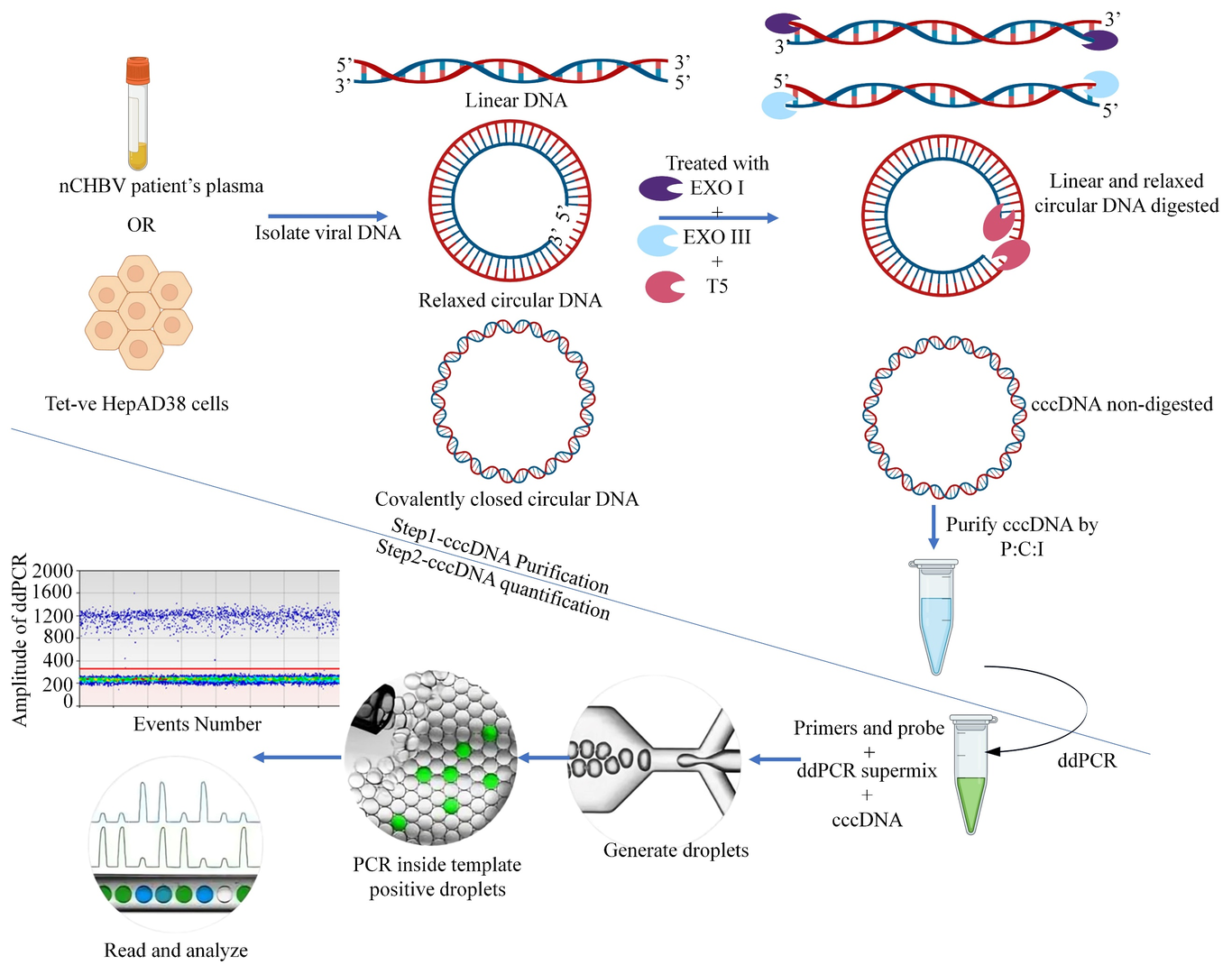
Covalently closed circular DNA (cccDNA) is a stable, episomal form of HBV DNA. cccDNA is a true marker for the intrahepatic events in controlled CHB infection. Quantifying cccDNA is critical for monitoring disease progression and efficacy of anti-viral therapies. To standardize the method, total HBV DNA was isolated from HepAD38 cells and digested with three exonuclease enzymes to remove linear and relaxed circular HBV DNA. Purified cccDNA quantification used ddPCR with specific primers. Treatment-naive chronic hepatitis B virus patients (nCHBV, n=36) with detectable HBV DNA and HBsAg, were grouped by HBsAg levels: Group I (HBsAg lo < 2000 IU/ml, n=11) and Group II (HBsAg hi > 2000 IU/ml, n=25). cccDNA, HBV DNA and HBsAg, were quantified in plasma and compared between groups. Correlation with clinical/histopathological features was done. Non-digested 3.6 ^10 6 tet -ve HepAD38 cells showed 316 copies/µl of total viral DNA. After digesting the linear, integrated, and relaxed circular DNA with triple enzymes, 15 copies/µl of cccDNA were detected. Similarly, after DNA digestion, HBsAg lo patients showed a median of 8.5 copies/µl (IQR 2.75-9.75 copies/µl), and HBsAg hi gave a median of 11 copies/µl (IQR 4-16 copies/µl) but with no significant difference between groups (p=0.093). Further, HBsAg lo patients with low cccDNA copy numbers showed significantly higher fibrosis grades than HBsAg hi (p=0.036). We conclude that employing a combined approach utilizing three exonucleases, cccDNA-specific primers, and ddPCR enables the detection of cccDNA copies even in patients exhibiting low levels of HBsAg and HBV DNA. This integrated method offers additional validation as a surrogate diagnostic tool.