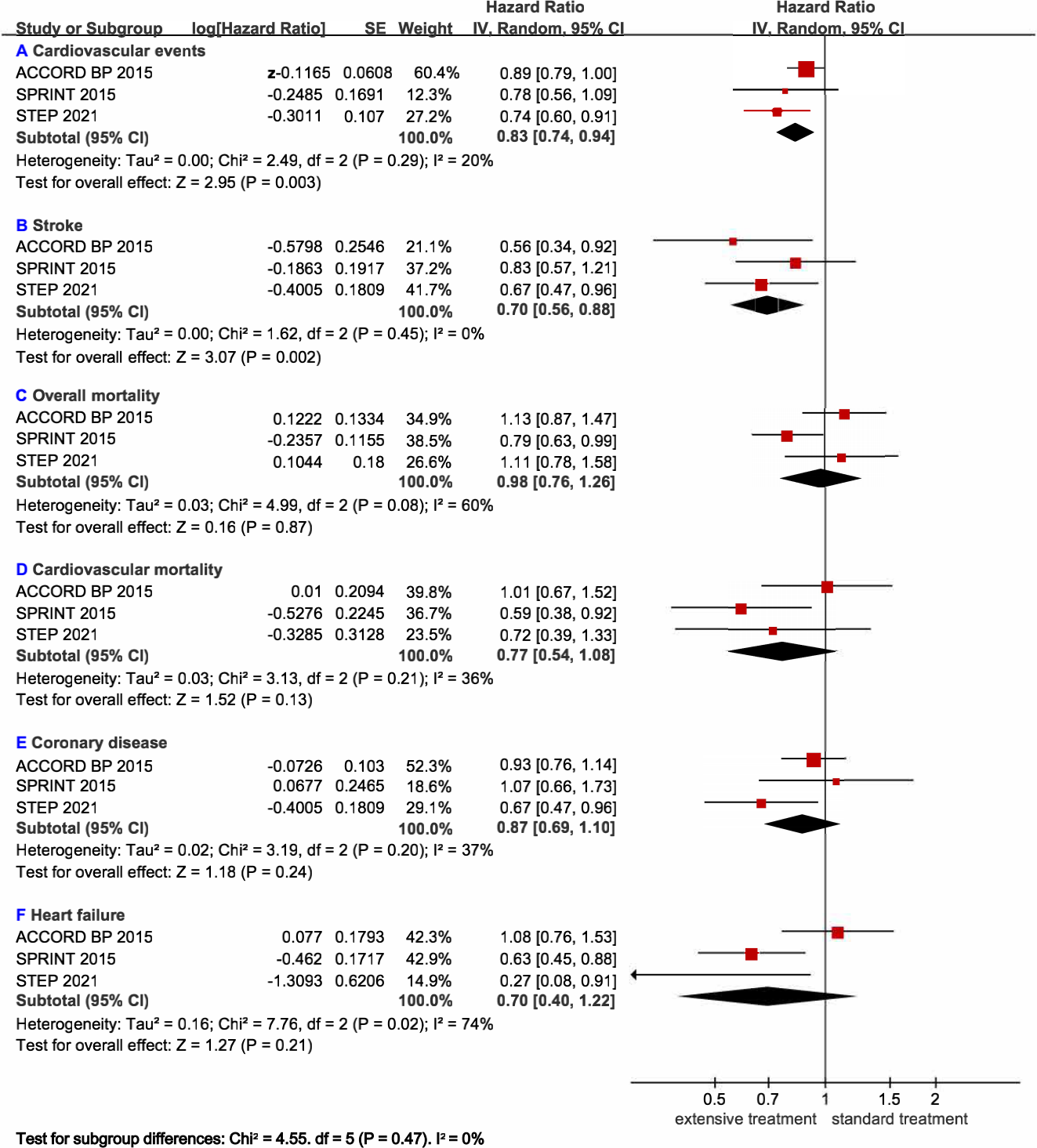
Abstract Aim: Blood pressure-lowering treatment is beneficial for preventing cardiovascular disease risk among elderly patients. However, the most appropriate BP targets for elderly patients are controversial. Methods: We extracted the individual-level data of participants over 60 years from the SPRINT study and ACCORD study first and then conducted a meta-analysis of major adverse cardiovascular events (MACEs) and adverse events (hypotension and syncope) and renal outcomes across the SPRINT, STEP, and ACCORD BP trials, which included 18,806 participants over 60. Participants were randomized to receive standard BP treatment or intensive BP treatment. Results: In this meta-analysis, intensive treatment exhibited a nominal trend toward decreases in all-cause death (hazard ratio [HR]: 0.98; 95% confidence interval [CI]: 0.76-1.26; p=0.87) and cardiovascular mortality (HR: 0.77; 95%CI: 0.54-1.08; p=0.13). The incidence of MACEs (HR: 0.83; 95%CI: 0.74-0.94; p=0.003) and stroke (HR: 0.70; 95% CI: 0.56-0.88; p=0.002) was reduced. Intensive treatment had an inconspicuous effect on coronary disease (HR: 0.87; 95% CI: 0.69-1.10; p=0.24) and heart failure (HR: 0.70; 95%CI: 0.40-1.22; p=0.21). Intensive treatment increased the risk of hypotension (HR: 1.46; 95%CI: 1.12-1.91; p=0.006) and syncope (HR: 1.43; 95%CI: 1.06-1.93; p=0.02). Intensive treatment did not increase the risk of either impaired kidney function among patients with chronic kidney disease (CKD) (HR: 0.98; 95% CI: 0.41-2.34; p=0.96) or without CKD (HR: 1.77; 95%CI: 0.48-6.56; p=0.40) at baseline. Conclusions: Intensive BP goals reduced the incidence of MACEs and increased the risk of adverse events without significant mortality or renal outcome changes.