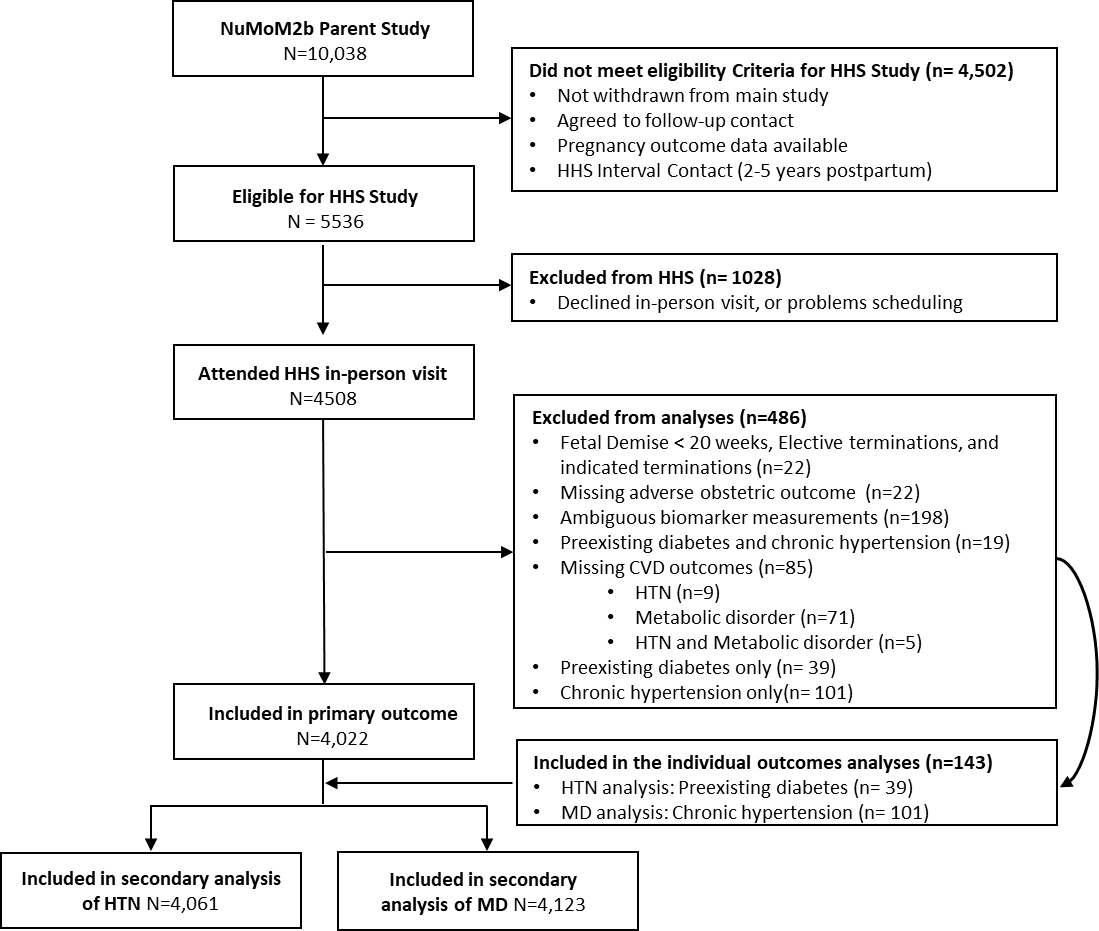
OBJECTIVE To assess the relationship between allostatic load in early pregnancy and CVD, 2 to 7 years postpartum, and potential pathways contributing to racial disparities in CVDs. DESIGN Secondary analysis of an observational cohort study. SETTING nuMom2b Heart Health Study. POPULATION Pregnant individuals. METHODS Our primary exposure was dichotomous high allostatic load in the first trimester, defined as four or more out of 12 biomarkers in the “worst” quartile. The primary outcome was new diagnosis of composite CVD, consisting of HTN and or MD (fasting glucose greater than 100 mg/dL or medication for diabetes). Each outcome and allostatic load component was analyzed secondarily. Multivariable logistic regression was used to test the association between high allostatic load and CVD adjusted for potential confounders. Mediation and moderation analyses assessed the role of high allostatic load in racial disparities of CVD. MAIN OUTCOME MEASURE Composite CVD. RESULTS Among 4,022 individuals, CVD was identified in 1,462 (36.4%); 26.6% had HTN, and had 15.4% MD. High allostatic load was present in 33.0%. After adjustment for covariates, high allostatic load was associated with CVD (aOR 2.0, 1.8-2.3), HTN (2.1, 1.8-2.4), and MD (1.7, 1.5-2.1). There was a reduction in the magnitude of the relationship between race and CVD with the addition of allostatic load. Self-reported race did not significantly moderate the relationship between allostatic load and CVD. CONCLUSION High allostatic load is associated with CVD. Allostatic load was a partial mediator between race and CVD. Race did not moderate the relationship between allostatic load and CVD.