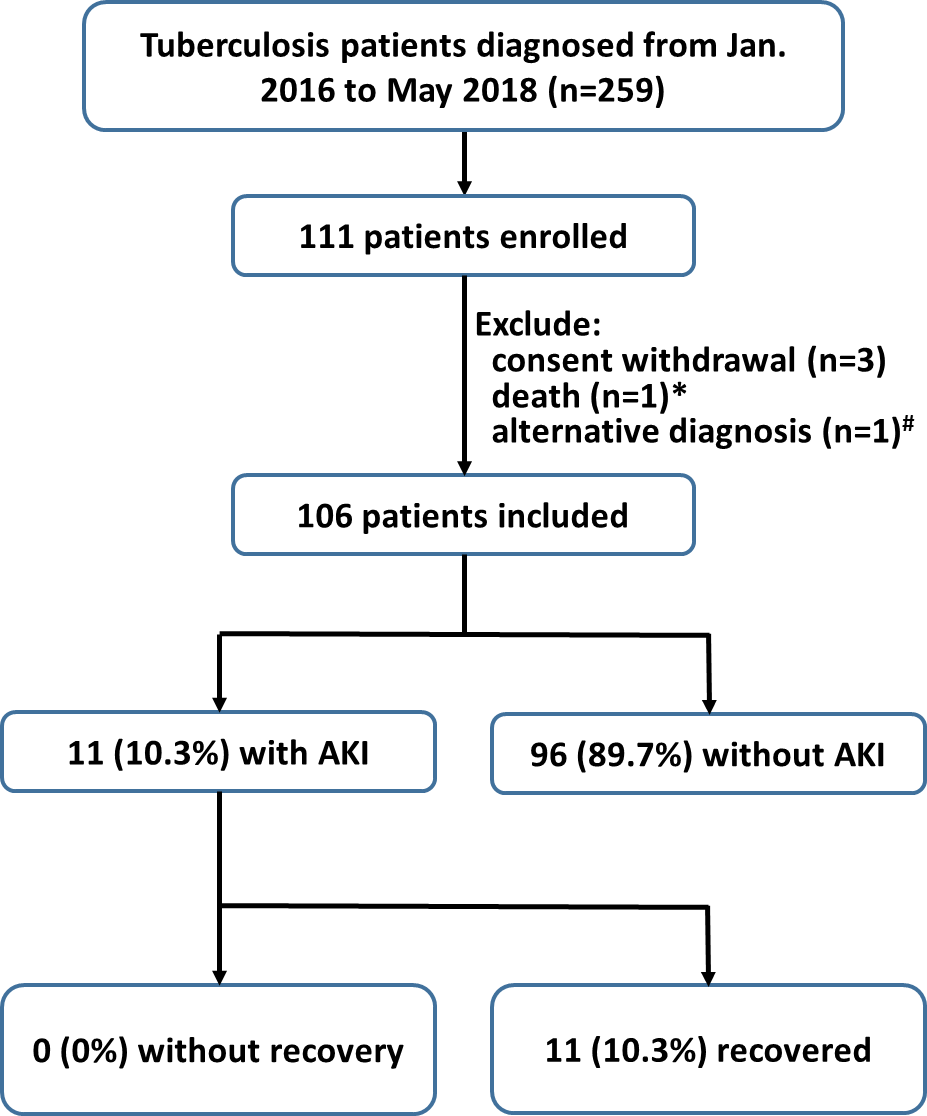
Aims: Acute kidney injury (AKI) is occasionally detected in patients receiving anti tuberculosis (TB) treatment. This prospective cohort study is the first to investigate the true incidence, risk factors, and renal outcomes. Methods: This study was conducted from January 1, 2016, to May 31, 2018, and patients with a new diagnosis of TB and receiving standard anti-TB treatment were enrolled; the patients received regular laboratory monitoring. AKI was defined according to the Kidney Disease: Improving Global Outcome (KDIGO) criteria. Urinalysis, measurements for blood erythrocyte morphology and the fractional excretion of sodium, and renal ultrasonography were performed at AKI onset. Anti-TB drugs were adjusted by the primary physician. Risk factors for AKI were identified using a Cox regression analysis. Results: In total, 106 patients were recruited (mean age: 52.6 years, 71.7% men). Eleven (10.3%) patients experienced AKI. An increase in serum uric acid and hemoglobin levels was noted at AKI onset. All patients with AKI exhibited renal function recovery and completed rifampin-containing anti-TB treatment. Age (hazard ratio (HR): 1.06 [1.02–1.11]), a higher baseline estimated glomerular filtration rate (eGFR; HR: 1.04 [1.02–1.06]), and a blood eosinophil count >350 (109/L) (HR: 10.99 [2.28–53.02]) were associated with AKI development during anti-TB treatment. Conclusions: Under regular pharmacovigilance monitoring, the incidence of renal function impairment during anti-TB treatment was higher than expected. AKI frequently occurred in older patients with a higher eGFR and blood eosinophil count. However, the complication had no influence on anti-TB treatment completion, and no permanent renal impairment occurred.