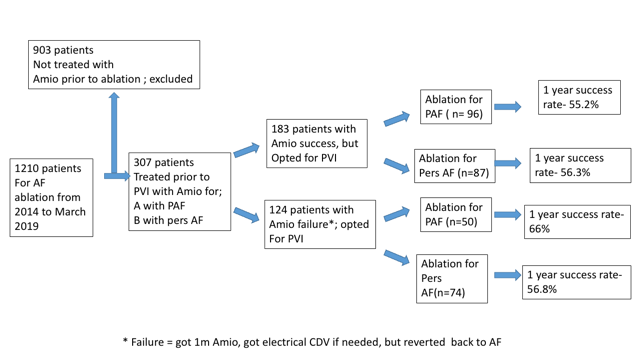
Background: Catheter ablation for atrial fibrillation (AF) is a common therapeutic strategy for patients with either paroxysmal or persistent AF, but long-term ablation success rates are imperfect. Maintenance of sinus rhythm immediately prior to ablation with anti-arrhythmic drug (AAD) therapy has been associated with improved outcomes in patients undergoing ablation. Amiodarone has superior efficacy relative to other AADs. Whether failure of amiodarone to maintain sinus rhythm prior to ablation for either paroxysmal or persistent AF is associated with poor outcomes is unknown. Methods: A total of 307 patients who received amiodarone in a one-year window before undergoing catheter ablation for AF were included. Patients were divided into amiodarone success (n=183) and amiodarone failure (n=124) groups based on the response to pre-ablation amiodarone treatment. Analysis of procedural outcomes as a function of response to amiodarone therapy was performed. Patients were followed for at least 12 months post-ablation to assess outcomes (adverse events and arrhythmia recurrence). Procedural success was defined by the absence of documented arrhythmia (>30s) without any anti-arrhythmic agents beyond a 90d blanking period. Results: Following ablation for either paroxysmal or persistent AF, freedom from any recurrent atrial arrhythmia at 1y was 57.7% for the entire cohort. One-year freedom from recurrent arrhythmia in the amiodarone success group was comparable to that in the amiodarone failure group (55.7% vs 60.5%; p=0.54). Success rates following ablation did not vary by the response to amiodarone when analyzed for paroxysmal or persistent AF subgroups. Conclusion: Failure to restore and maintain sinus rhythm with amiodarone prior to ablation for either paroxysmal or persistent AF is not a predictor of ablation procedural failure. Amiodarone failure alone should not deter practitioners from considering ablation therapy for patients with AF.