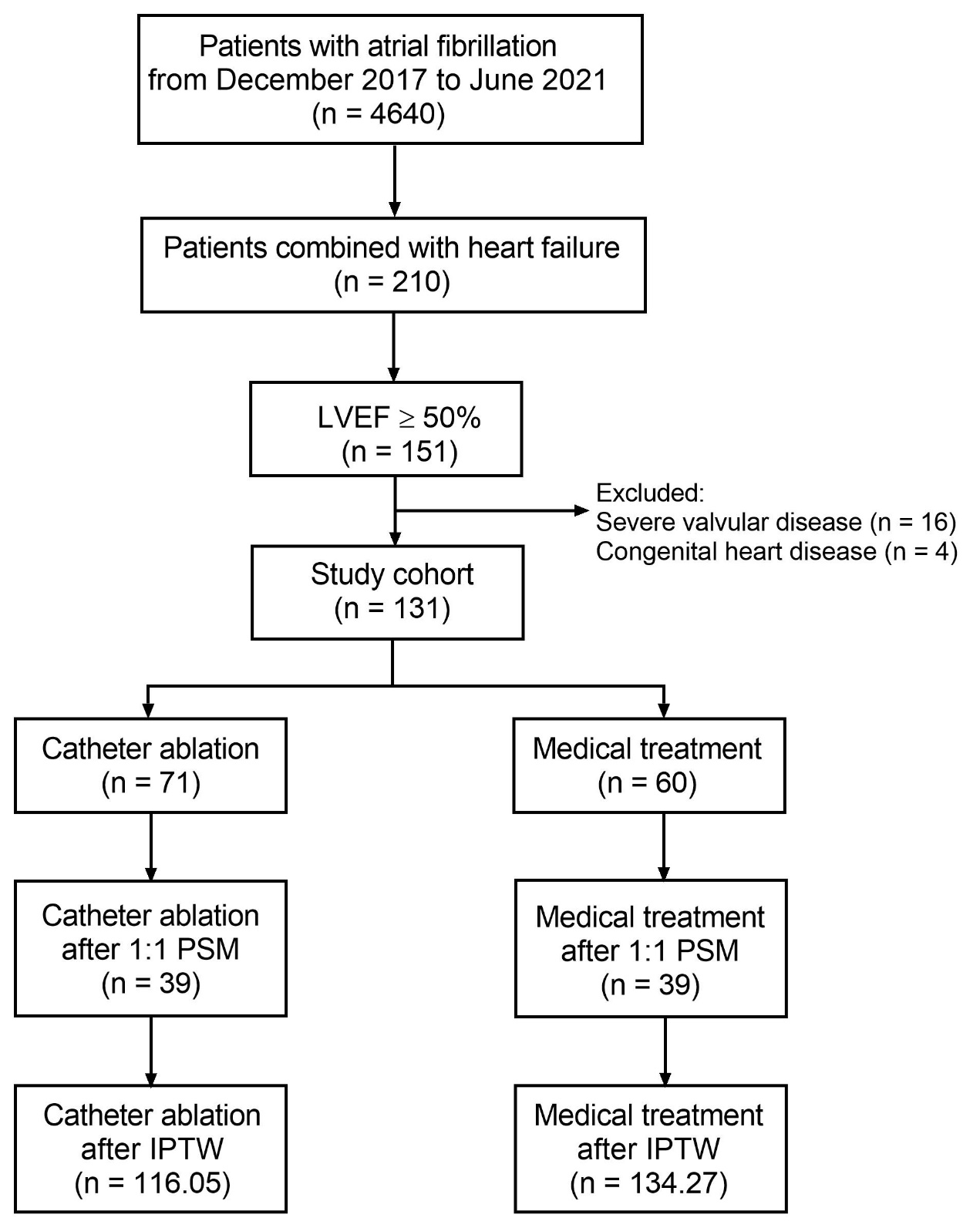
Background We aimed to compare the long-term outcomes of catheter ablation and medical treatment in patients with atrial fibrillation (AF) and heart failure with preserved ejection fraction (HFpEF). Methods We retrospectively screened consecutive patients with AF and HFpEF who received catheter ablation or medical treatment from December 2017 to June 2021 in our institution. The primary endpoint was defined as a composite of all-cause death, thromboembolic events and heart failure (HF) hospitalization. Multivariate analysis, 1:1 propensity score matching (PSM) and inverse probability of treatment weighting (IPTW) were employed to adjust for potential confounders. Results A total of 131 patients were included, among whom 71 patients (54.2%) underwent 1.15 + 0.36 catheter ablation procedures. During a median follow-up of 31.8 months, the incidence of the primary endpoint was significantly lower in catheter ablation group (9.9% vs 25.0%, log rank p = 0.018) compared with medical treatment group. In the multivariate model, catheter ablation was independently associated with a lower incidence of the primary endpoint (hazard ratio 0.281, 95% confidence interval 0.110 – 0.721, p = 0.008), which was consistent both in PSM and IPTW cohorts. The New York Heart Association class [2 (1, 2) vs 2 (2, 2), paired p < 0.001], N-terminal pro-B type natriuretic peptide level [334.3 (187.1, 821.8) vs 859.2 (308.4, 1903.0), paired p < 0.001] and left atrial diameter (39.4 + 6.4 vs 41.1 + 6.2, paired p = 0.001) were significantly improved at the end of follow-up in catheter ablation group. Conclusion Catheter ablation was significantly associated with a lower incidence of the composite endpoint, improved HF symptoms and reverse atrial remodeling in AF and concomitant HFpEF.