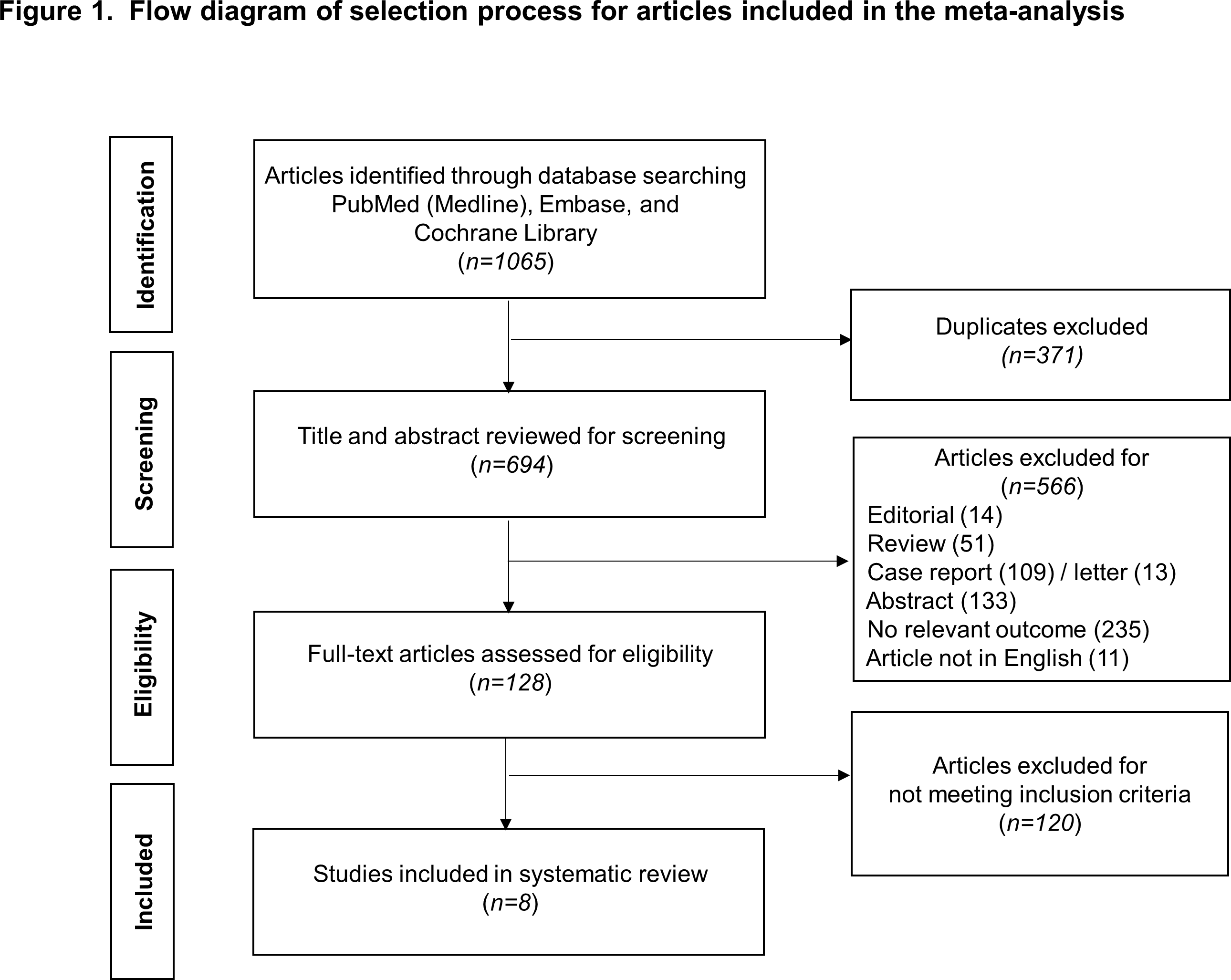
Background: Although the beneficial effects of cardiac resynchronization therapy (CRT) in heart failure (HF) are fully established in HF with left ventricular ejection fraction (LVEF) ≤ 35%, CRT strategy for HF with mildly reduced ejection fraction (HFmrEF) is controversial. Left bundle branch area pacing (LBBAP) is an emerging pacing modality and an alternative option to CRT, and the efficacy and safety are promising so far. The aim of this analysis was to perform a systematic review of the literature and meta‐analysis on impact of LBBAP strategy in HFmrEF, with LVEF between 35 % and 50%. Methods: PubMed, Embase, and Cochrane Library were searched for full-text articles on LBBAP from inception to July 17, 2022. The outcomes of interest were QRS duration, and LVEF at baseline and at follow-up in mid-range HF. Data were extracted and summarized. A random-effect model incorporating the potential heterogeneity was used to synthesize the results. Results: Out of 1065 articles, 8 met the inclusion criteria for 211 mid-range HF patients with an implant LBBAP across the 16 centers. The average implant success rate with lumenless pacing lead use was 91.3%, and 19 complications were reported among all 211 enrolled patients. During the average follow-up of 9.1 months, average LVEF were 39.8% at baseline and 50.5% at follow-up (MD: 10.90%, 95% CI: 6.56 - 15.23 P<0.01). Average QRS duration were 152.6ms at baseline and 119.3ms at follow-up (MD: -34.51ms, 95% CI: -60.00 to -9.02, P < 0.01). Conclusion: LBBAP could significantly reduce QRS duration and improve systolic function in patient with LVEF between 35 and 50%. Application of LBBAP as a CRT strategy for heart failure with mildly reduced ejection fraction may be a viable option.