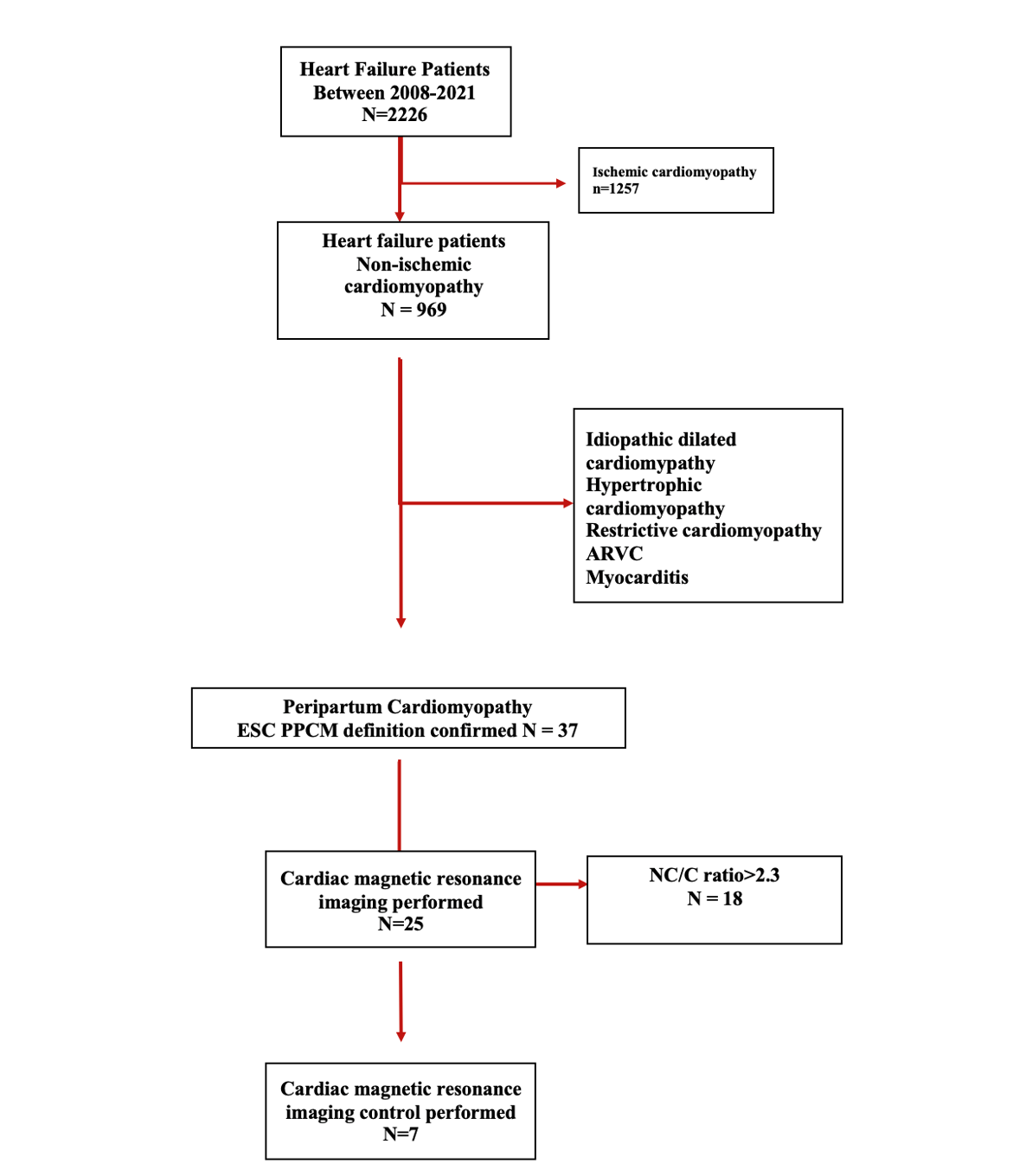
Objective: Peripartum cardiomyopathy (PPCM) diagnosis made by excluding identifiable causes of heart failure (HF) and occurs end of the pregnancy or during the postpartum period of five months. It presents a clinical HF spectrum with left ventricular systolic dysfunction. Background: The purpose of this study is to retrospectively evaluate the clinical characteristics, cardiac magnetic resonance (CMR) imaging features, and end-points consisting of left ventricle recovery, left ventricular assist device implantation, heart transplantation, and all-cause mortality. Method: Outpatient HF records between 2008 to 2021 were screened. Thirty-seven patients were defined as PPCM. Twenty-five patients had CMR evaluation at the time of diagnosis, and six patients were re-evaluated with CMR. Results: The mean age was 30.5±5.6 years, and the mean LVEF was 28.2±6.7%. In thirteen(35.7%) patients, LVEF recovered during the follow-up course. The median recovery time was 281(IQR [78-358]) days. LVEF on CMR was 35.3±10.5, and three patients exhibited late gadolinium enhancement(LGE) patterns. Sub-endocardial and mid-wall uptake pattern types were detected. 18(75%) patients met the Petersen left ventricle non-compaction cardiomyopathy(LVNC) criteria. Patients with NC/C ratio lower than 2.3 had lower LVEDVi and LVESVi (124.9±35.4,86.4±7.5, p=0.003;86.8±34.6,52.6±7.6, p=0.006), respectively. The median follow-up time was 2129 (IQR [911-2634]) days. The primary endpoint-free one-year survival was 88.9%(event rate 11.1%), and five-year survival was 75.7%(event rate 24.3%). Conclusion: In a retrospective cohort of PPCM patients, 35.7% of patients’ LVEF recovered, and the primary end-point of free-five-year survival was 75%. Twenty-five patients were assessed with CMR; three of four met the Petersen CMR-derived LVNC at initial evaluation.