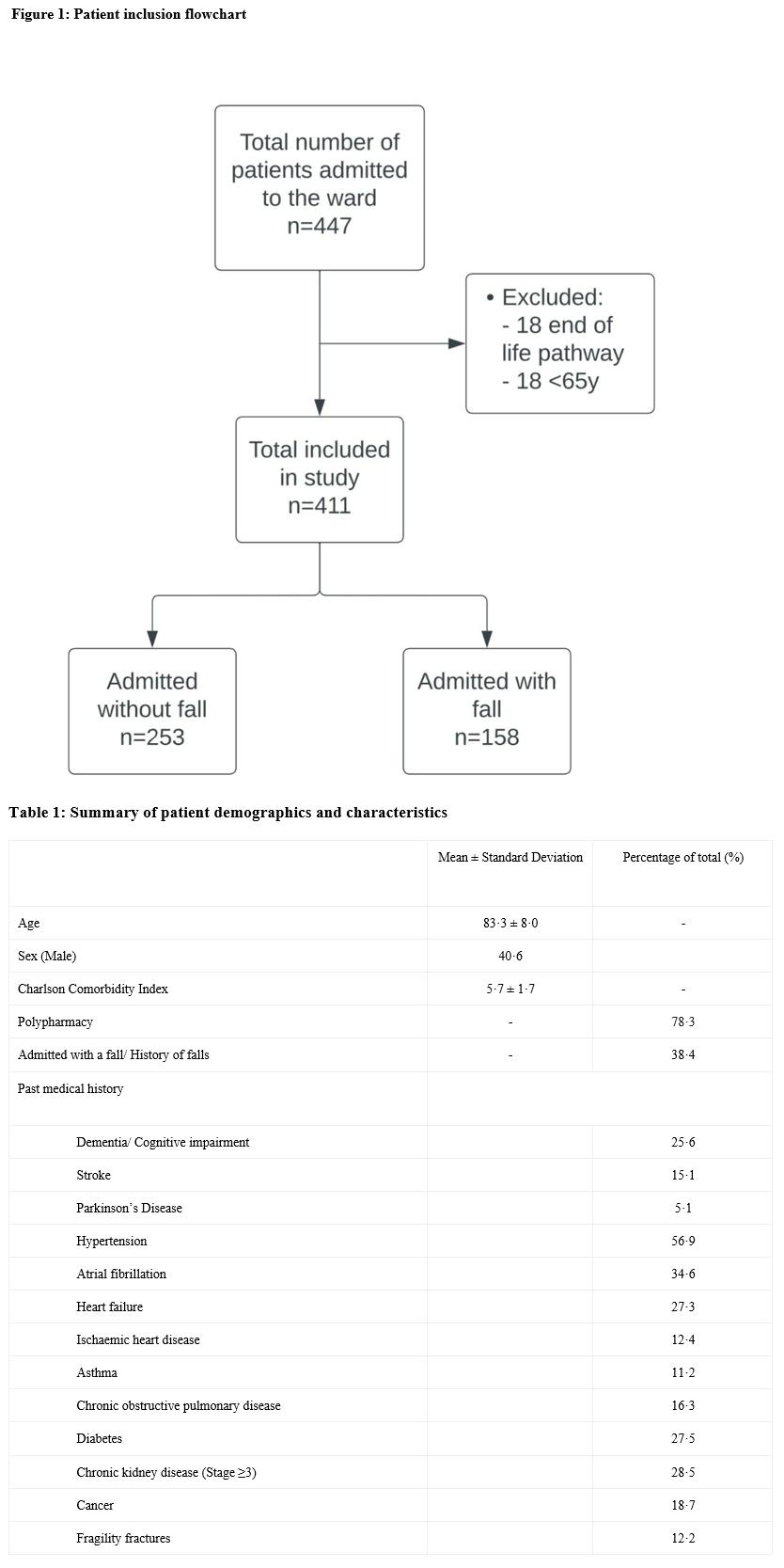
Background and Purpose Polypharmacotherapy is a growing phenomenon associated with adverse effects in older adults. We assessed the potential confounding effects of cumulative anticholinergic burden (ACB) in patients who were hospitalised with falls. Methods A non-interventional, prospective cohort study of unselected, acute admissions aged ≥65 years. Data were derived from electronic patient health records. Results were analysed to determine the frequency of polypharmacotherapy and degree of ACB and their relationship to falls risk. Primary outcomes were polypharmacotherapy, defined by ≥5 medications, and ACB score. Key Results 411 consecutive subjects were included, mean age 83·8 ± 8·0 years: 40·6% male. 38·4% were admitted with fall. Incidence of polypharmacotherapy was 80·8%, (88·0% and 76·3% among those admitted with and without fall respectively). Incidence of ACB score of 0, 1, 2, ≥3 was 38·7%, 20·9%, 14·6% and 25·8% respectively. On multivariate analysis, age (OR=1·03, [1·0 ; 1·05], p= 0·0494), ACB score (OR=1.15, [1.02 ; 1.29], p= 0.0245), polypharmacotherapy (OR=2·14, [1·19 ; 3·87], p= 0·0115) but not Charlson Comorbidity Index (OR=0·92, [0·81 ; 1·04], p= 0·1723) were significantly associated with higher falls rate. Of patients admitted with fall, 29·8% had drug-related orthostatic hypotension, 24·7% had drug-related bradycardia, 37·3% were prescribed centrally acting drugs and 12·0% were taking inappropriate hypoglycaemic agents. Interpretation Polypharmacotherapy results in cumulative ACB and both are significantly associated with falls risk in older adults. The presence of polypharmacotherapy and each unit rise in ACB score have a stronger effect of increasing falls risk compared to age and comorbidities.