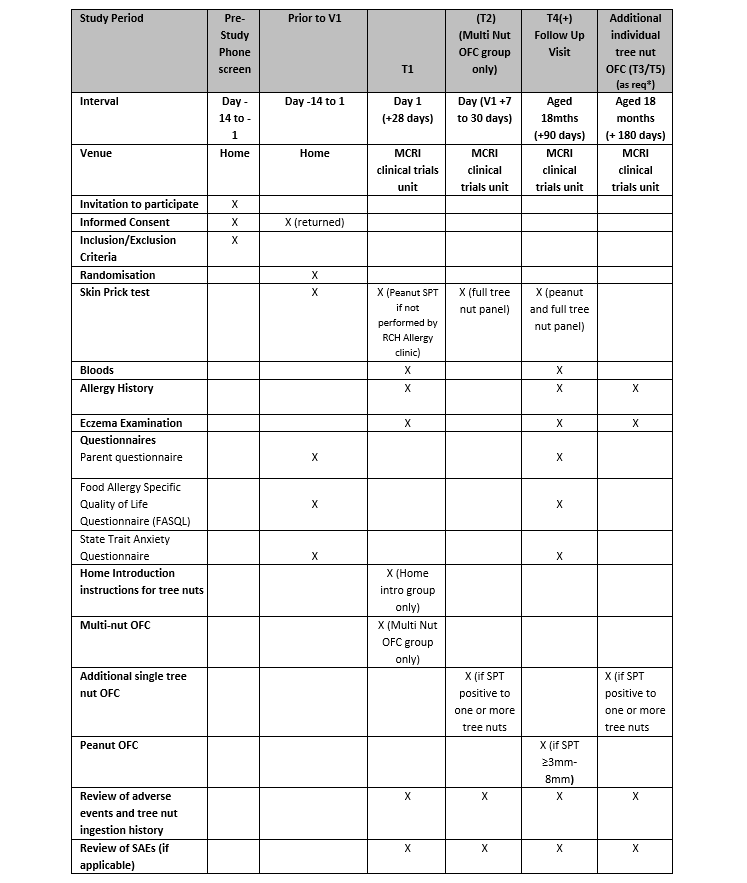
Introduction: Children with peanut allergy are at increased risk of developing tree nut allergies, which can be severe and for most lifelong. Introduction of peanut in the first year of life can reduce the risk of peanut allergy, however, prevention strategies for tree nut allergies have not been established. We aimed to test the efficacy and safety of a novel strategy, a supervised multi-nut oral food challenge (OFC) compared to standard care for tree nut allergy prevention in infants at high risk of developing tree nut allergy, TreEAT. Methods and analysis: TreEAT is a 2-armed, open-label, randomised, controlled trial (RCT). Infants (n=212) aged 4-11months with peanut allergy will be randomised 1:1 at peanut allergy diagnosis to either a hospital-based multi-tree nut (almond, cashew, hazelnut and walnut) OFC using multi-nut butter or standard care (home introduction of individual tree nuts). All infants will be assessed at age 18months, with questionnaires and SPT to peanut and tree nuts. Peanut and tree nut OFCs will be performed as required to determine allergy status for each nut. The primary outcome is tree nut allergy at age 18 months. Secondary outcomes include peanut allergy resolution, proportion and severity of adverse events related to tree nut ingestion, number and frequency of tree nuts ingested, quality of life and parental anxiety and allergy related healthcare visits from randomisation to 18 months of age. Analyses will be performed on an intention-to-treat basis. Ethics and dissemination TreEAT was approved by the Royal Children’s Hospital Human Research Ethics Committee (#70489). Outcomes will be presented at scientific conferences and disseminated through publication. Trial registration number: ClinicalTrials.gov ID: NCT04801823