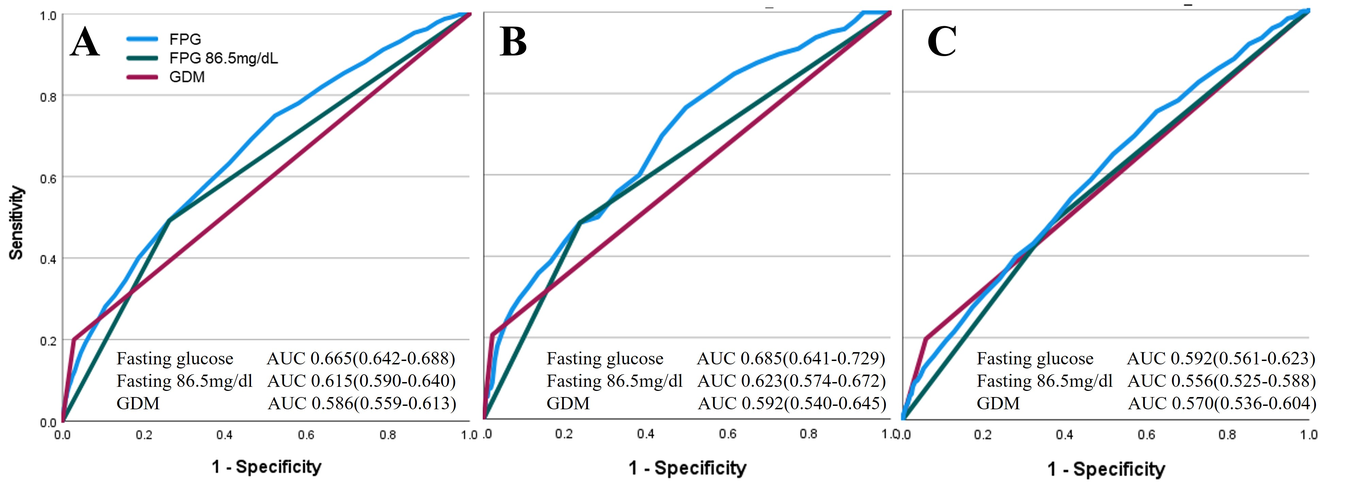
Objective: To evaluate the prediction performance of 1st trimester fasting plasma glucose (FPG) levels, as compared to gestational diabetes (GDM), for type 2 diabetes mellitus (T2DM), in a 5-year follow-up after pregnancy. Design: A retrospective analysis of prospectively collected data Setting: Mehuedet HMO, Israel Population or sample: 69,001 parturients with FPG levels measured at 1st-trimester and T2DM data up to 5 years after delivery. Methods: T2DM diagnosis was stratified by FPG levels divided into categories with 10 mg/dl increments. GDM was diagnosed using the two-step strategy. Prediction performance for T2DM was determined using ROC-AUC statistics with the utilization of the Youden index(YI) for the calculation of the best FPG cut-off for T2DM prediction. Survival analysis was applied to calculate hazard ratios(HRs) for T2DM prediction with further stratification to maternal obesity status. Main outcome measures: T2DM, as determined by the Israeli National Diabetes Registry.. Results: The determined FPG cut-off for predicting the risk of T2DM was 86.5mg/dl (sensitivity 53.3%, specificity 72.4%). This cutoff demonstrated superior predictive performance when compared to GDM diagnosis (0.615 vs. 0.586). Furthermore, all FPG level categories exceeding 80 mg/dL were associated with an increased risk of developing T2DM. FPG levels equal to or greater than 110 mg/dL exhibited even stronger predictive performance for T2DM compared to GDM diagnosis (HR 4.92 and 3.92, respectively). When stratified by maternal obesity, FPG levels displayed enhanced predictive capabilities for T2DM, particularly among women without obesity. Conclusions: 1st trimester FPG levels are associated with increased risk for T2DM, at least as GDM.