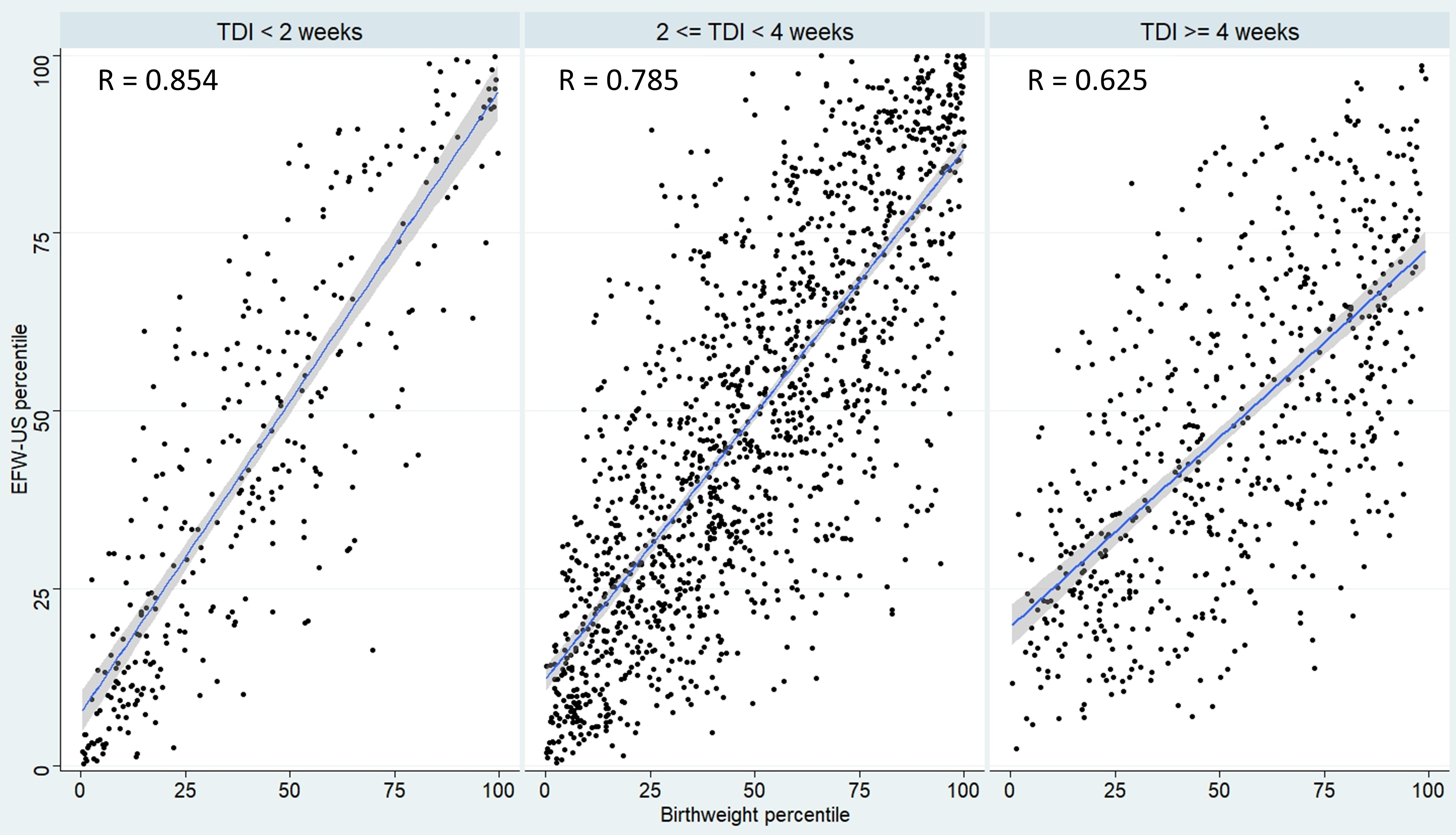
Objective: To assess the influence of the test-to-delivery interval (TDI) on the performance of ultrasound (US) and magnetic resonance imaging (MRI) for predicting birthweight (BW). Design: Secondary analysis of a prospective cohort study. Setting: Belgium, 2016. Population: Women with singleton pregnancy and live birth who underwent estimated fetal weight (EFW) by US and MRI between 36 +0/7 and 36 +6/7 weeks of gestation (WG). Methods: The study population was grouped into three groups: TDI<2 weeks (group 1, n=313), TDI≥2 and <4 weeks (group 2, n=1440), and TDI≥4 weeks (group 3, n=625). Main outcome measures The correlation between EFW-US or EFW-MRI and BW as well as the performance of both tests in predicting BW>95 th, >90 th, <10 th, and <5 th percentiles according to TDI. Results: There was a strong positive correlation between MRI-EFW and BW percentiles in group 1 (R=0.934 [95%CI: 0.918-0.947]), it dropped significantly but remained strongly positive in groups 2 and 3 (p<0.001). In contrast, the correlation between US-EFW and BW percentiles was highly positive only in group 1, and significantly lower than that of MRI-EFW/BW percentiles among the three groups (p<0.001). At the upper extreme of BW percentiles, MRI had a higher sensitivity with higher threshold of EFW percentile at a fixed false positive rate of 5%, in comparison to US regardless of TDI. Conclusions: The performance of MRI in the prediction of BW is maximal when the delivery occurs within two weeks of the examination, declining slowly thereafter, in contrast to the performance of US which decreases drastically over time.