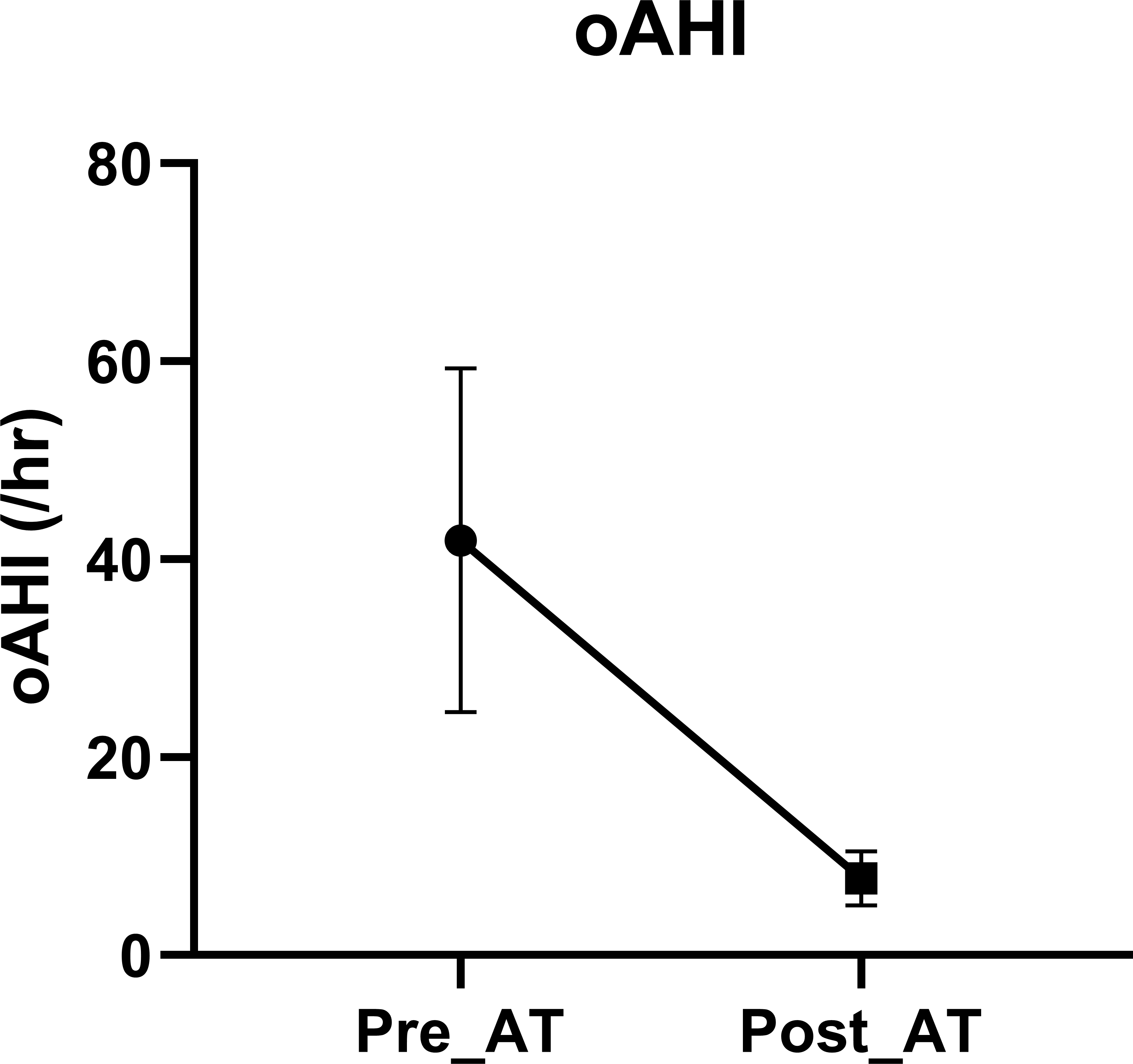
Introduction Children with Down Syndrome (DS) are at high risk of sleep disordered breathing (SDB). We aimed to examine the burden of SDB in infants with DS referred to tertiary sleep center. Methods Infants (≤12 months old) with DS who underwent consecutive polysomnography (PSG) at a single academic sleep center over a 6-year period were included. OSA (obstructive apnea hypopnea index [oAHI]>1/hr), central sleep apnea (central apnea index>5/hr) and the presence of hypoventilation (% time spent with CO2 > 50 mmHg either by end-tidal or transcutaneous> 25% of total sleep time) and hypoxemia (time spent with O2 saturation <88% >5 min) were ascertained. For infants who underwent adenotonsillectomy (AT), we compared the SDB metrics before and after the AT. Results A total of 40 infants were included (Mean age 6.6 months, male 66%). PSGs consisted of diagnostic (n=13) and split night (n=27, 68%) studies. All met criteria for OSA with mean oAHI 34.6 (32.3). Central sleep apnea was present in 11 (27.5%) of infants. A total of 11 (27.5%) had hypoxemia. Hypoventilation was present in 10 (25%) infants. There was a trend of association between hypothyroidism and hypoventilation (OR: 5.5 [0.96-34.4], p=0.056). Among 13 infants who underwent AT and had a follow up PSG, severity of OSA markedly reduced after AT (oAHI difference: 34/hr [29], p=0.0002). Conclusion This study highlights the high prevalence of SDB in infants with DS and supports early PSG assessment in this patient population.