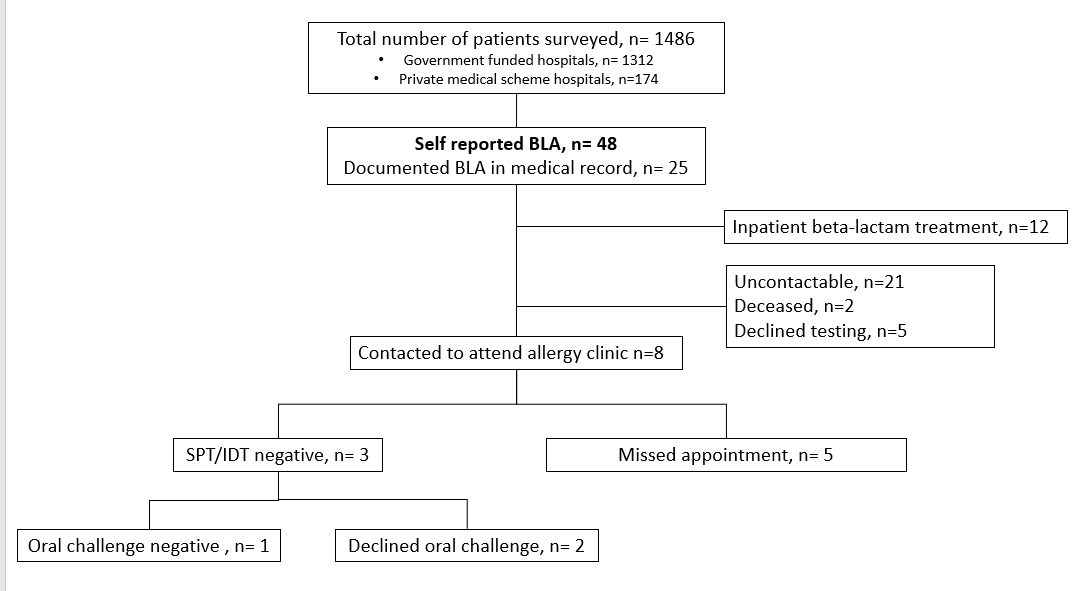
Background Up to a quarter of inpatients in high-income countries self-report beta-lactam allergy (BLA), which if incorrect, can increase use of alternative antibiotics that impact on bacterial resistance.. The epidemiology of BLA in low- and middle-income African countries is unknown. Methods Point-prevalence surveys were conducted at seven hospitals (adult, pediatric, government and private-funded, district- and tertiary-level) in Cape Town, South Africa between April 2019 and June 2021. Ward prescription records and interviews were conducted to identify BLA patients. De-labeling was attempted at the tertiary allergy clinic at Groote Schuur hospital. Findings A total of 1486 hospital inpatients were surveyed (1166 adults; 308 children). Only 48 (3.2%) patients self-reported a BLA with a higher rate amongst private- versus government-funded hospitals [6.3% vs 2.8%, p=0.014]. Using the PEN-FAST tool, only 10.4% (5/48) of self reported BLA patients were classified as high risk for true penicillin hypersensitivity. Antibiotics were prescribed to 70.8% (34/48) of self reported BLA patients, with 64.7% (22/34) receiving a beta-lactam. Despite three attempts to contact patients for de-labelling at the allergy clinic, only 3/36 underwent in vivo testing, with no positive results and one patient proceeded toa negative oral challenge. Interpretation Unlike high-income countries, self-reported BLA is low amongst inpatients in South Africa. The majority of self-reported BLA were low risk for type 1 hypersensitivity, but out-patient de-labeling efforts were largely unsuccessful. Funding None