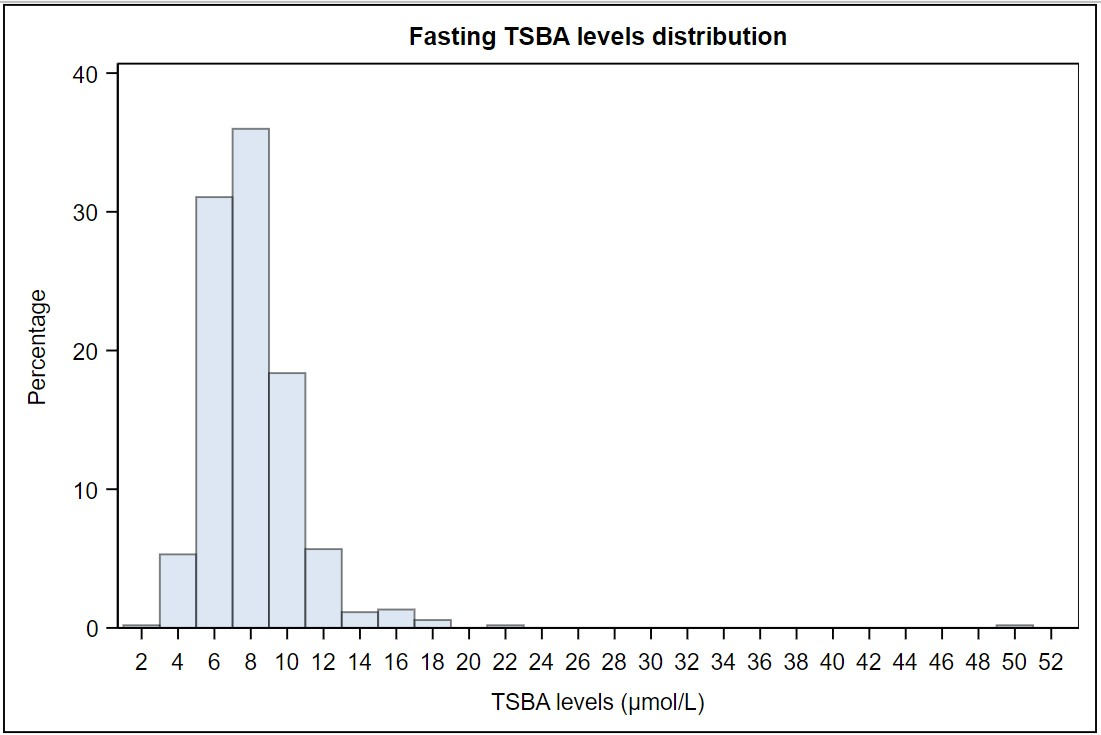
Objective To establish pregnancy-specific reference ranges for fasting and postprandial total serum bile acids (TSBA) levels. Design Cross-sectional study. Setting Tertiary care university hospital. Population Healthy pregnant women at term admitted to the Obstetrics Department over one year. Exclusion criteria were an established diagnosis of intrahepatic cholestasis of pregnancy (ICP) or any co-existing condition of increased risk for ICP. Methods and Main Outcome Measures Both fasting and postprandial TSBA levels were measured in 612 women (528 fasting and 377 postprandial samples). Results Reference intervals of 4.4-14.1 µmol/L for fasting TSBA, and 4.7-20.2 µmol/L for postprandial TSBA were established. The postprandial values were significantly higher than the fasting measurements, with a mean increase of 1.77 µmol/L (22%). A correlation between fasting TSBA levels and postprandial levels was found, as well as with fetal gender, parity, and the use of assisted reproductive technologies. A seasonal pattern was noticed for both fasting and postprandial TSBA, with the highest values in the winter season (p < 0.01 and 0.02, respectively). Conclusions Normal pregnancy is a sub-cholestatic state and is associated with a physiological elevation of TSBA levels, therefore a higher threshold should be considered for the diagnosis of ICP. We suggest using the upper reference limit observed in our healthy pregnant population (fasting ≥14 µmol/L and postprandial ≥20 µmol/L). As the fasting measurement is more specific for the diagnosis, and the postprandial is essential for severity assessment, it is recommended to measure both values, rather than use random samplings. Funding No funding to declare.