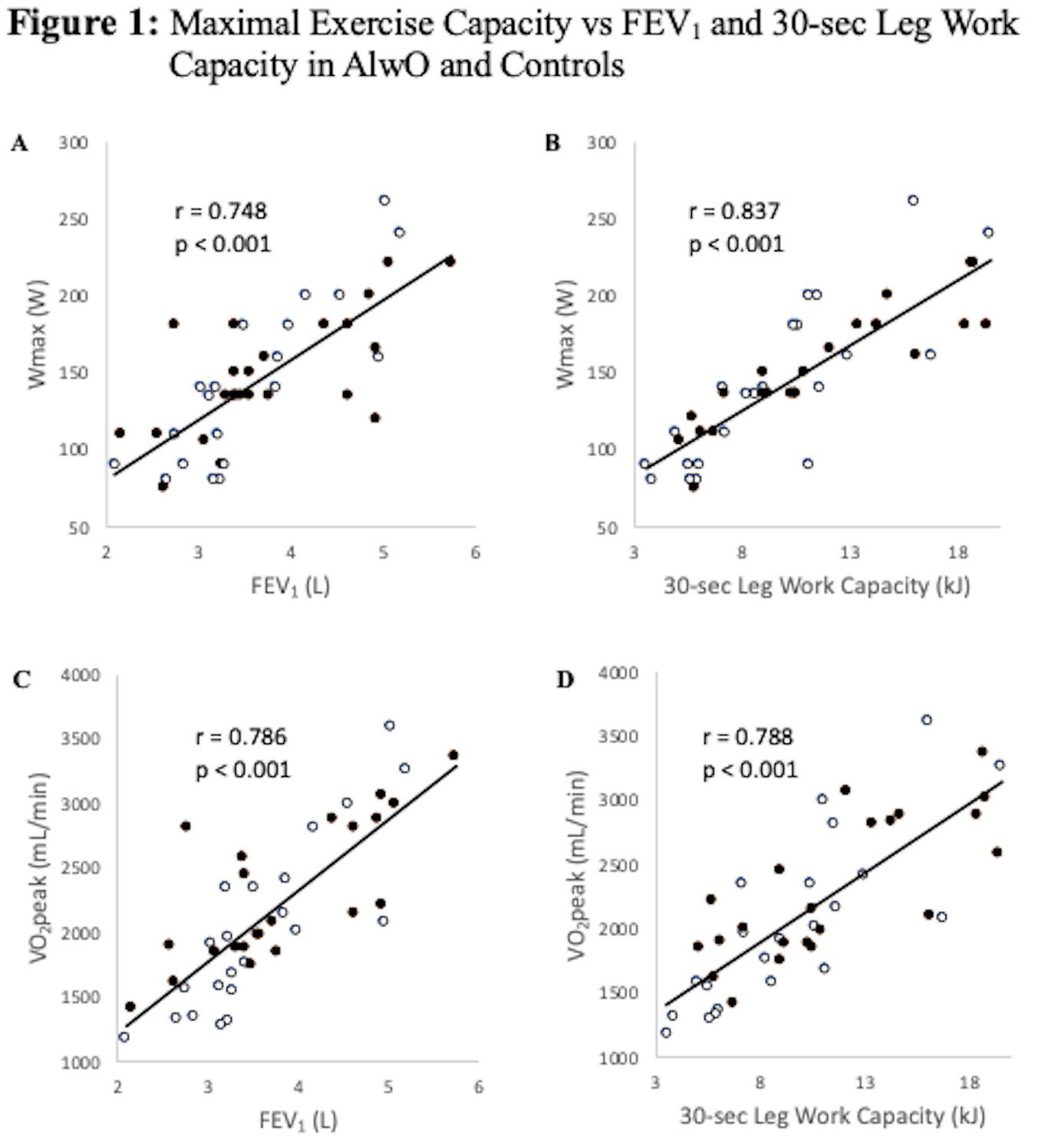
Background Adolescents living with obesity (AlwO) can have limited exercise capacity. Exercise capacity can be predicted by a 2-factor model comprising lung function and leg muscle function, but no study has looked at cycling leg muscle function and its contribution to cycling exercise capacity in AlwO. Methods 22 nonobese adolescents and 22 AlwO (BMI>95 percentile) were studied. Anthropometry, body composition (DEXA), spirometry, 30-sec isokinetic work capacity, and maximal exercise (cycle ergometry) were measured. Results AlwO had greater lean leg mass (LLM) (14.8±4.1 vs 21.0±4.3 kg, Con vs AlwO p<0.001). Lung function did not differ, although FEV 1 trended higher in AlwO (101.0±13.1 vs 107.9±12.7 percent predicted, p=0.08). Leg 30-second work output did not differ in absolute terms or per allometrically scaled LLM. Peak oxygen consumption did not differ between the groups in absolute terms or as percent predicted values (78.5±15.4 vs 82.1±16.5 percent predicted), but was lower in AlwO when expressed per scaled kg of LLM. Peak oxygen consumption related to both lung function and 30-second work capacity, with no observed group effect. 30-second leg work capacity related to the scaled muscle mass, with a small group effect. There was some correlation between leg work capacity and time spent in moderate to vigorous physical activity in AlwO (r s=0.39, p=0.07). Conclusion AlwO have larger LLM and preserved exercise capacity, when expressed as percentage of predicted, but not per allometrically scaled LLM. Increasing time spent in moderate to vigorous activity may benefit AlwO.