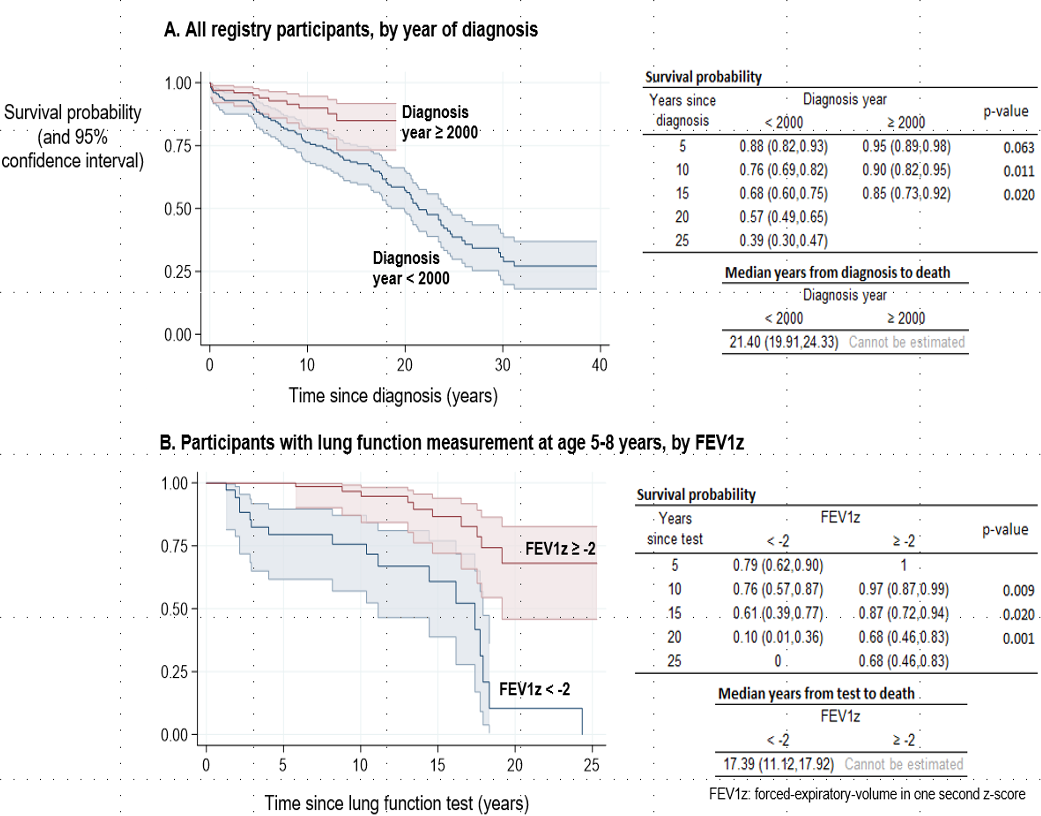
Introduction: Temporal trends in CF survival from low-middle-income settings are poorly reported. We describe changes in CF survival after diagnosis over 40 years from a South African (SA) CF center. Methods: An observational cohort study of people diagnosed with CF from 1974 to 2019. Changes in age-specific mortality rates from the year 2000 (versus before 2000) were estimated using multivariable Poisson regression. Data were stratified by current age < or ≥ 10 years and models controlled for diagnosis age, sex, ethnicity, genotype, and P. aeruginosa (PA) infection. A second analysis explored association of mortality with weight and FEV1z-scores at age 5-8 years. Results: 288 people (52% male; 57% Caucasian; 44% p.Phe508del homozygous) were included (median diagnosis age 0.5 years: Q1,Q3: 0.2, 2.5); 58 (35%) died and 30 (10%) lost to follow-up. Among age >10 years, age-specific mortality from year 2000 was significantly lower (adjusted hazard ratio aHR: 0.14; 95% CI: 0.06,0.29; p<0.001), but not among age <10 years (aHR: 0.67; 95% CI: 0.28,1.64; p=0.383). In children <10 years, Caucasian ethnicity was associated with lower mortality (aHR 0.17; 95% CI 0.05,0.63), and time since first PA infection with higher mortality (aHR 1.31; 95% CI 1.01,1.68). Mortality was 7-fold higher if FEV1z was < -2.0 at age 5-8 years (aHR 7.64; 95% CI 2.58,22.59). Conclusion: Overall, CF survival has significantly improved in SA from year 2000 in people older than 10 years. However, increased risk of mortality persists in young non-Caucasian children, and with FEV1z<-2.0 at age 5-8 years.