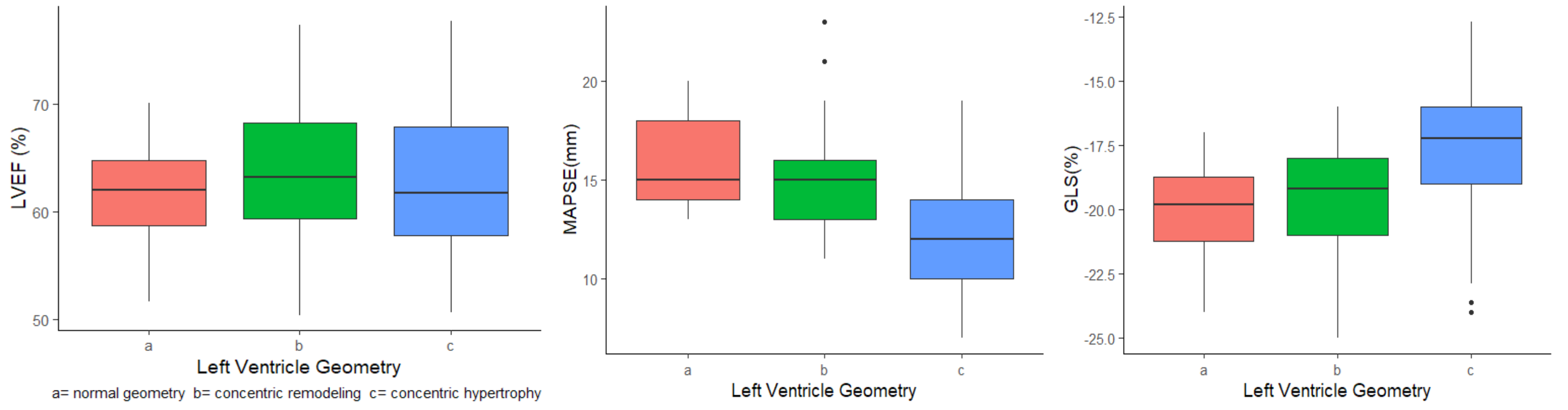
Background: The left ventricle (LV) journey in their transition from hypertrophy to heart failure is marked by many subcellular events partially understood yet. The moment in which the structural abnormalities reach the umbral to induce myocardial dysfunction remains elusive. Aims: To evaluate the anatomic-functional relationship between LV wall thickness and longitudinal systolic dysfunction. Material and Methods: We prospectively performed clinical history and transthoracic echocardiogram on healthy individuals and patients with hypertension, left ventricle ejection fraction (LVEF) ≥50%, and absence of heart failure symptoms. Results: A total of 226 patients and 101 healthy individuals were recruited. The distribution for sex was similar between groups. The mean age was 67±13 years old in the patients, and 44% had concentric LV hypertrophy. LVEF was identical in both groups (63±6%); in contrast, global longitudinal strain (GLS) (-18.8±2.5% vs. -20.4±2%) and mitral annulus plane systolic excursion (MAPSE) (13.8±2.8 vs. 15.5±2mm) were lower. ROC curve classified optimally decreased GLS with LV septum thickness ≥13mm and decreased MAPSE with thickness ≥14mm. Multivariable logistic regression found that LV septum thickness is the only variable associated with longitudinal systolic dysfunction (OR= 1.1, CI95%= 1.05 – 1.15, p= 0.001, R squared= 0.38). Discussion: A progressive increase in LV wall thickness due to myocyte hypertrophy and interstitial expansion is associated with LV systolic longitudinal dysfunction. Conclusions: Patients with moderate or severe ventricular hypertrophy (septum ≥13mm) had longitudinal systolic dysfunction, GLS decreases with minor structural change than MAPSE, and LVEF is insensitive in detecting longitudinal myocardial dysfunction in patients with hypertension.