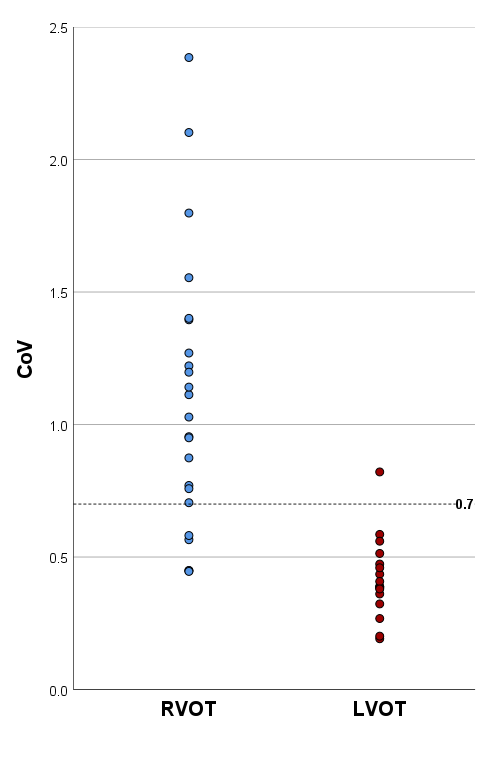
Introduction: Prior to ablation, predicting the site of origin (SOO) of outflow tract ventricular arrhythmia (OTVA), can inform patient consent and facilitate appropriate procedural planning. We set out to determine if OTVA variability can accurately predict SOO. Methods: Consecutive patients with a clear SOO identified at OTVA ablation had their prior 24-hour ambulatory ECGs retrospectively analysed (derivation cohort). Percentage ventricular ectopic (VE) burden, hourly VE values, episodes of trigeminy/bigeminy, and the variability in these parameters were evaluated for their ability to distinguish right from left sided SOO. Effective parameters were then prospectively tested on a validation cohort of consecutive patients undergoing their first OTVA ablation. Results: High VE variability (coefficient of variation ≥ 0.7) and the presence of any hour with < 50 VE, were found to accurately predict RVOT SOO in a derivation cohort of 40 patients. In a validation cohort of 29 patients, the correct SOO was prospectively identified in 23/29 patients (79.3%) using CoV, and 26/29 patients (89.7%) using VE < 50. Including current ECG algorithms, VE < 50 had the highest Youden Index (78), the highest positive predictive value (95.0%) and the highest negative predictive value (77.8%). Conclusion: VE variability and the presence of a single hour where VE < 50 can be used to accurately predict SOO in patients with OTVA. Accuracy of these parameters compares favourably to existing ECG algorithms.