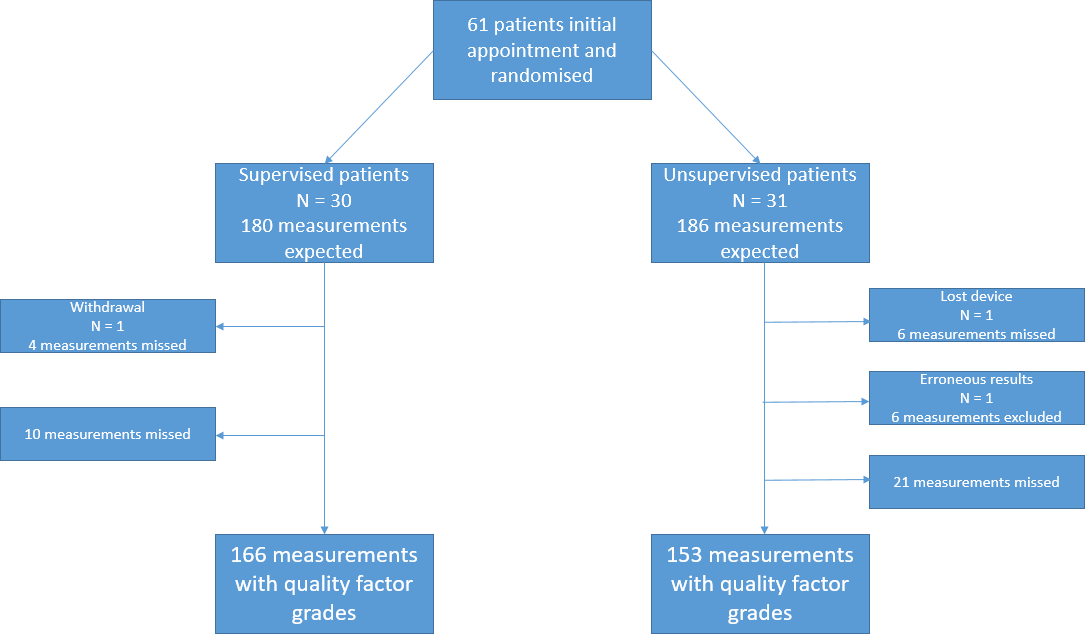
Introduction: The COVID-19 pandemic has accelerated the move towards home spirometry monitoring, including in children. Our aim was to determine whether the remote supervision of spirometry by a physiologist improves the technical quality and failure rate of the manoeuvres. Method: Children with cystic fibrosis who had been provided with NuvoAir home spirometers were randomly allocated to either supervised or unsupervised home spirometry following a detailed training session. Home spirometry was performed every 2 weeks for 12 weeks. Tests were assigned a quality factor (QF) using our laboratory grading system as per ATS/ERS standards, with tests marked from A to D, or Fail. In our laboratory we aim for QF A in all spirometry tests, but report results of QF B or C with a cautionary note. QF A was therefore the primary outcome, and QF A-C the secondary outcome. Results: 61 patients were enrolled; 166 measurements were obtained in the supervised group, and 153 in the unsupervised group. Significantly more measurements achieved QF A in the supervised compared to unsupervised group (89% vs 74%; p= <0.001) whilst proportions reaching grade A-C were similar (99% vs 95%; p=0.1). All significant declines in spirometry results had a clinical rather than technical reason. Family/patient feedback for both arms was very positive. Conclusion: These results suggest that home spirometry in children should ideally be remotely supervised by a physiologist, but acceptable results can be obtained if resources do not allow this, provided that training is delivered and results monitored according to our protocol.