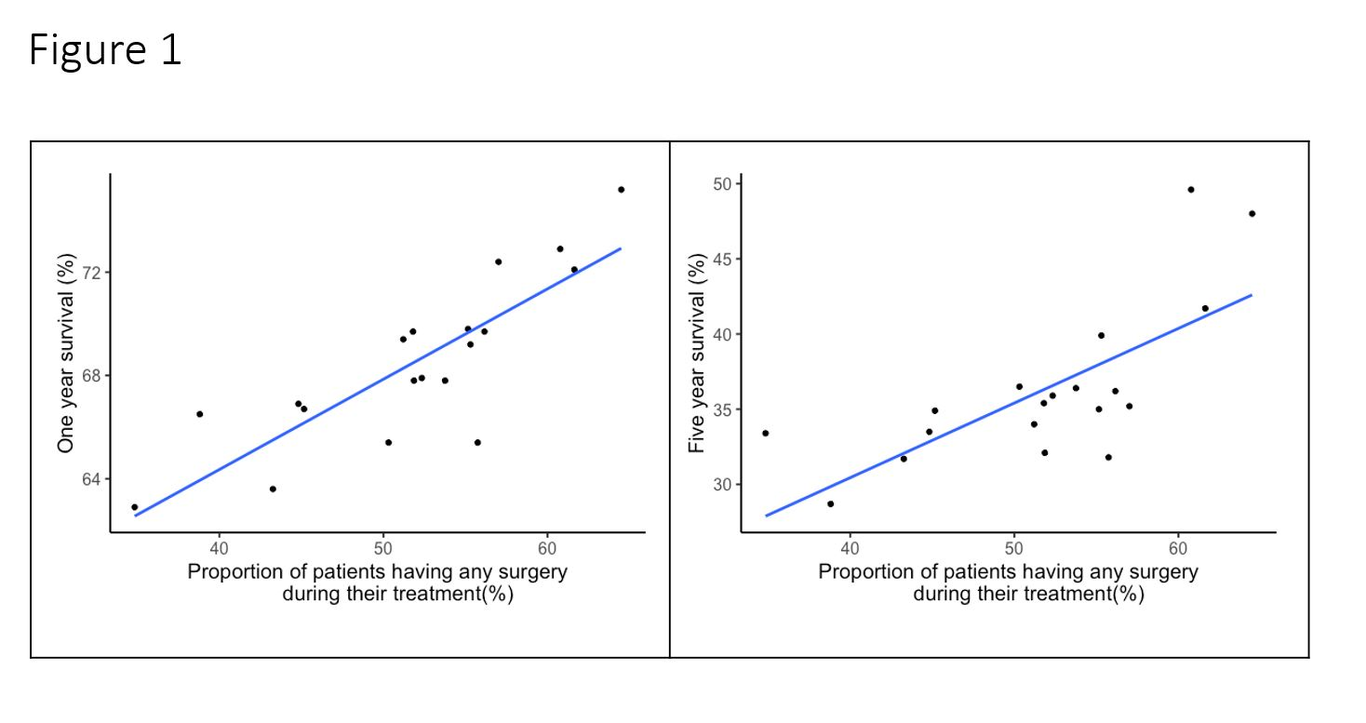
Objective The role of surgery for patients with advanced ovarian cancer is well established but wide variations in the percentage of patients undergoing surgery exist. Design Observational Study Setting The 19 cancer alliances in England, UK Methods We undertook a comparative analysis to examine the effects of rates of surgery on one and five year disease specific survival across the 19 English Cancer Alliances. We also undertook a propensity score analysis of a single cohort of patients with advanced ovarian cancer to compare patients who did, and did not, undergo surgery as part of their primary management. Main outcome measures Correlations between rates of surgery, demographics, and cancer alliance performance against one and five year survival Results In multivariable analysis, rates of surgery undertaken by a Cancer Alliance remained an independent predictor of both one and five year survival (correlation coefficient 0.81, and 0.70, respectively) although this relationship is likely non linear with optimal rates of surgery still to be defined. Using propensity score analysis a subgroup of patients who gain no benefit from surgery can be identified. Conclusions Overall survival of patients with advanced ovarian cancer is likely to be improved with an increase in overall rates of surgery however there are likely to be optimal maximal rates, above which patients will be disadvantaged. Mechanisms for identifying individual outcome predictions are required.