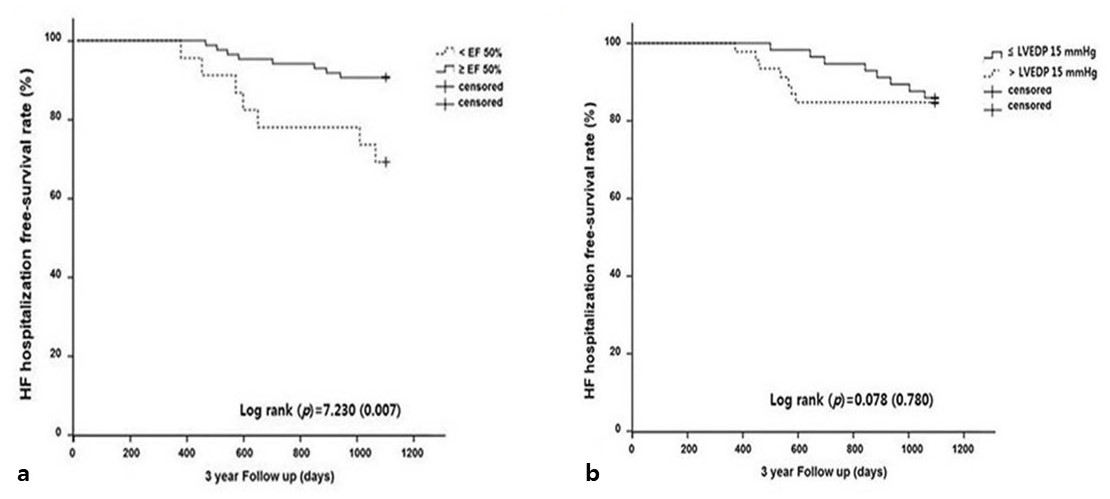
Objectives: Systolic and diastolic dysfunctions are related to adverse clinical outcomes in patients with sinus rhythm. The aim of this study was to clarify the prognostic significance of systolic and diastolic dysfunctions in patients with chronic persistent atrial fibrillation (AF). Methods: We evaluated data for 114 consecutive patients with chronic AF who underwent measurement of LVEDP at our hospital between 1 March 2011 and 31 December 2014. In total, 114 consecutive patients with chronic AF were divided into two groups according to the left ventricular ejection fraction (LVEF): LVEF < 50 (reduced ejection fraction, REF group) and LVEF ≥50 (preserved EF, PEF group). The PEF group was further divided into two subgroups according to the left ventricular end-diastolic filling pressure (LVEDP): LVEDP >15 mmHg and LVEDP ≤ 15 mmHg. The 3-year clinical outcomes were compared between the PEF and REF groups and the LVEDP ≥15 mmHg and LVEDP <15 mmHg groups. Results: During the 3-year follow-up period, the rate of heart failure (HF) hospitalisation and incidence of AF with rapid ventricular rhythm (RVR) were higher in the REF group than in the PEF group. Multivariate analysis revealed that REF was the only significant predictor of HF hospitalisation (hazard ratio, 4.71; 95% confidence interval, 1.48–15.02; p=0.009). Conclusions: Our observations during a mid-term follow-up period revealed that systolic dysfunction could be an important predictor of HF hospitalisation in patients with AF. However, elevated LVEDP may not be associated with mid-term adverse clinical outcomes in patients without systolic dysfunction.