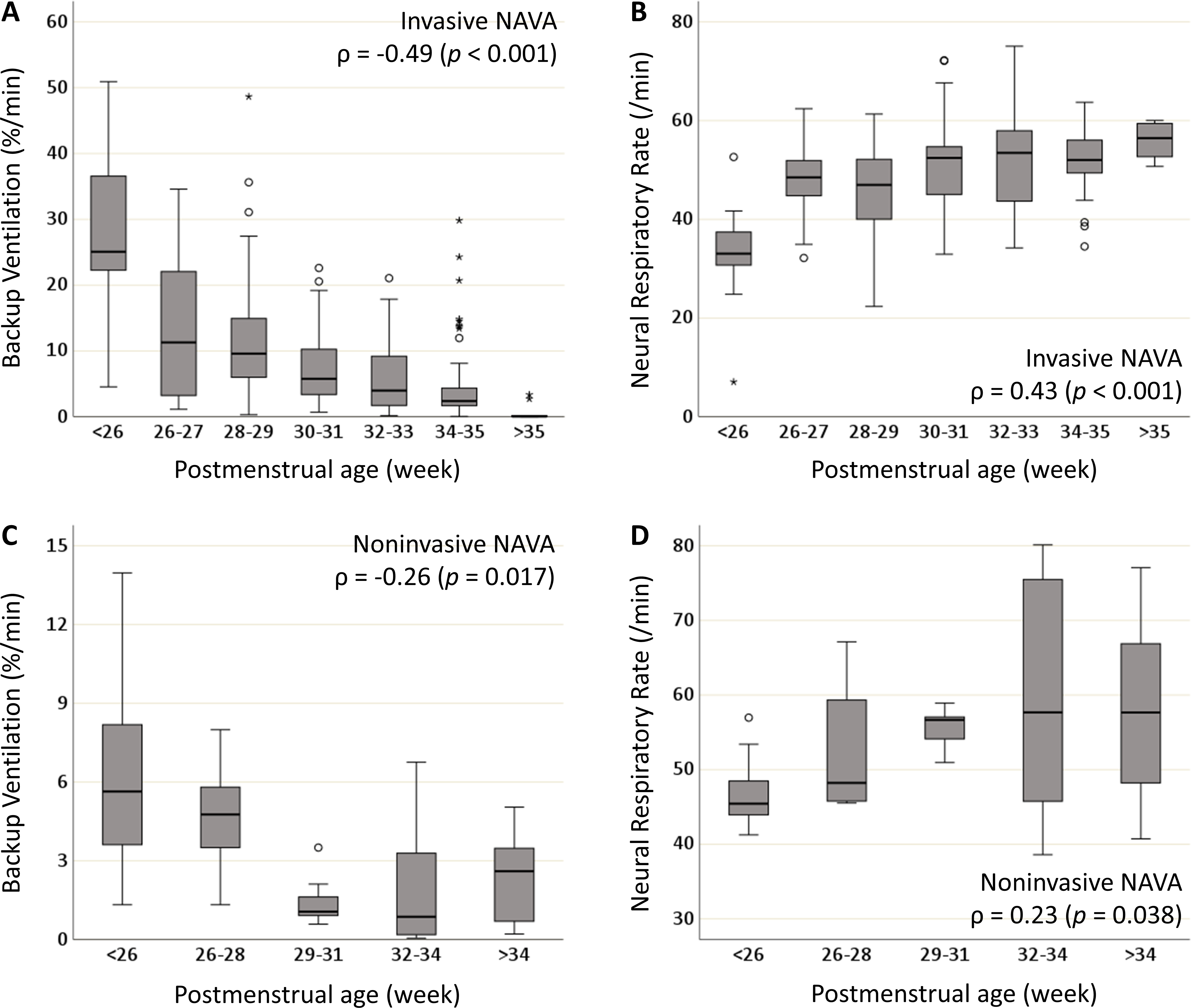
Objective: To analyze the proportion of backup ventilation during neurally adjusted ventilatory assist (NAVA) in preterm infants at different gestational ages and to analyze the trends in backup ventilation in relation to clinical deteriorations. Methods: A prospective observational study was conducted in 18 preterm infants born at a median (range) 27+4 (23+4–34+4) weeks of gestation with a median (range) birth weight of 1,100 (460–2,820) g, who received respiratory support with either invasive or noninvasive NAVA. Data on ventilator settings and respiratory variables were collected daily; the mean values of each 24-hour recording were computed for each respiratory variable. For clinical deterioration, ventilator data were reviewed at 6-hour intervals for 30 hours prior to the event. Results: A total of 354 ventilator days were included: 269 and 85 days during invasive and noninvasive NAVA, respectively. The time on backup ventilation (%/min) significantly decreased, and the neural respiratory rate increased with increasing postmenstrual age during both invasive and noninvasive NAVA. The median time on backup ventilation was less than 15%/min, and the median neural respiratory rate was more than 45 breaths/min for infants above 26+0 weeks of gestation during invasive NAVA. The relative backup ventilation significantly increased prior to the episode of clinical deterioration. Conclusion: The proportion of backup ventilation during NAVA showed how the control of breathing matured with increasing gestational age. Even the most immature infants triggered most of their breaths by their own respiratory effort. An acute increase in the proportion of backup ventilation anticipated clinical deterioration.