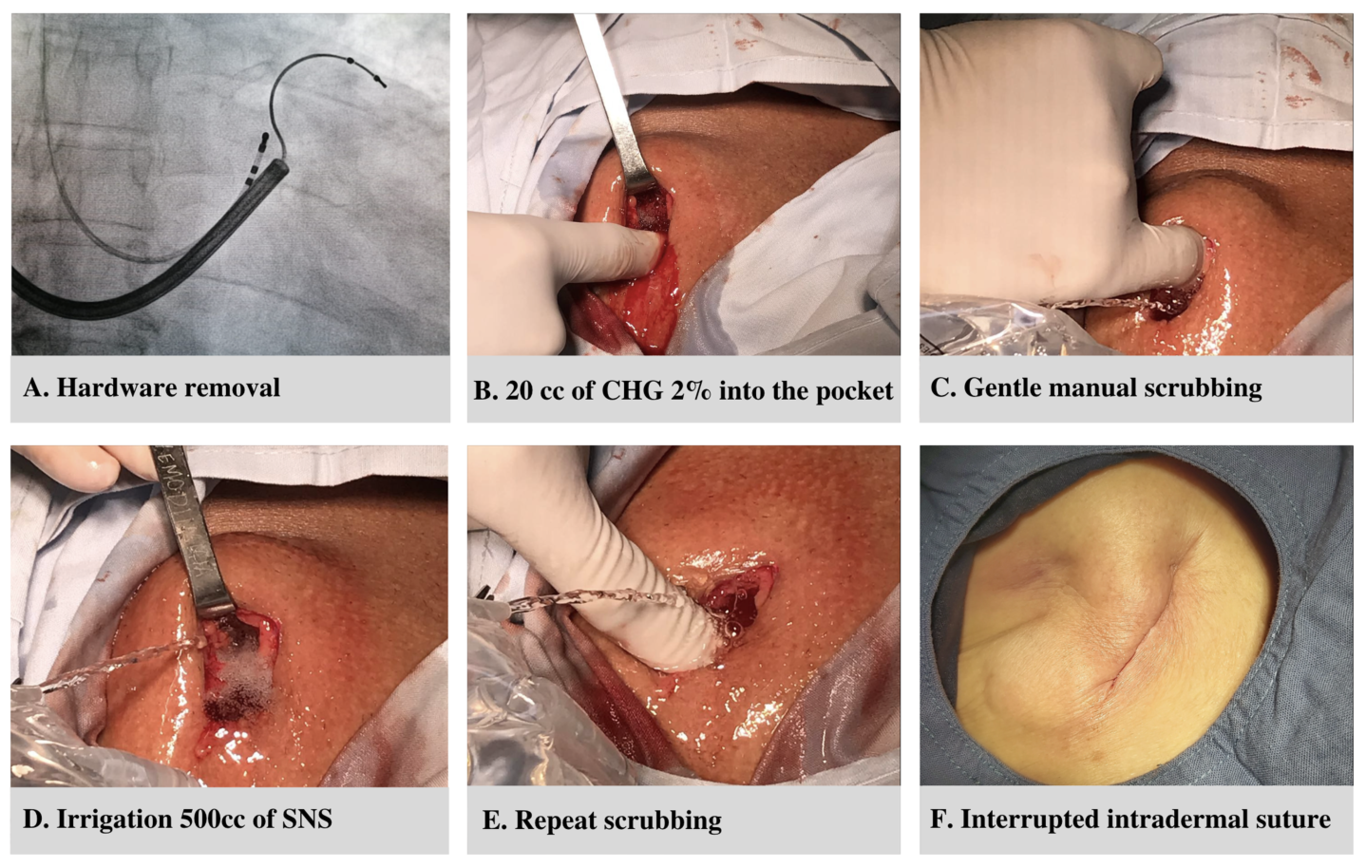
Introduction: Capsulectomy is recommended in patients with cardiac implantable electronic device (CIED) infection after transvenous lead extraction (TLE) but is time-consuming and requires extensive tissue debridement. In this study, we describe the outcomes of chlorhexidine gluconate (CHG) scrubbing in lieu of capsulectomy for the treatment of CIED infections. Methods: This retrospective observational study included patients who underwent TLE for CIED-related infections. In the capsulectomy group, complete capsulectomy was performed after hardware removal. In the CHG group, thorough scrubbing of the generator pocket with 20 cc of 2% CHG followed by irrigation with approximately 500 cc of sterile normal saline (SNS) was performed. The primary outcomes included reinfection and hematoma formation in the generator pocket. Secondary outcomes included any adverse reaction to chlorhexidine, the need for reintervention, infection-related mortality, and total procedural time. Results: A total of 102 patients (mean age 67.2±13 years, 32.4% female) underwent CIED extraction with either total capsulectomy (n=54) or CHG (n=48) scrubbing. Hematoma formation was significantly higher in the capsulectomy group vs. the CHG group (13% vs. 0%, p=0.014), with no significant differences in the reinfection rate. Capsulectomy was associated with longer procedural time (133.7±78.5vs. 89.9±51.8 minutes, p=0.002). No adverse reactions to CHG were found. Four patients (4.3%) died from worsening sepsis: 3 in the capsulectomy group and 1 in the CHG group (p=0.346). Conclusions: In patients with CIED infections, the use of CHG without capsulectomy resulted in a lower risk of hematoma formation and shorter procedural times without an increased risk of reinfection or adverse events associated with CHG use.