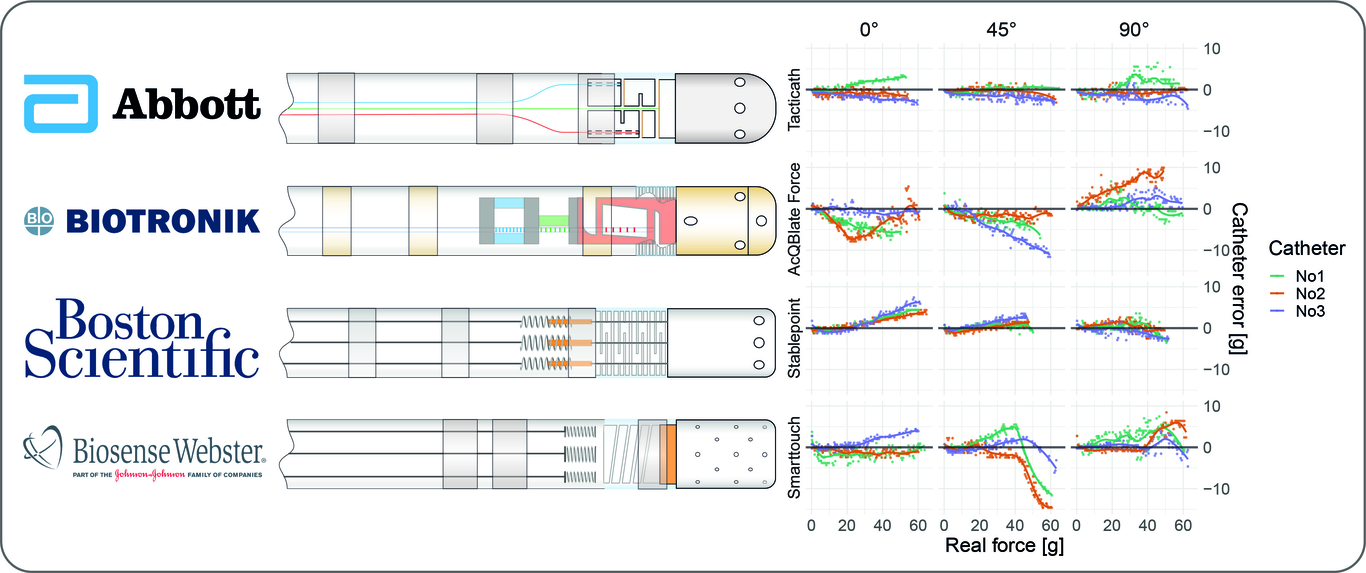
Introduction: Contact force-sensing catheters are widely used for ablation of cardiac arrhythmias. They allow quantification of catheter-to-tissue contact, which is an important determinant for lesion formation and may reduce the risk of complications. The accuracy of these sensors may vary across the measurement range, catheter-to-tissue angle, and amongst manufacturers and we aim to compare the accuracy and reproducibility of four different force sensing ablation catheters. Methods: A measurement setup containing a heated saline water bath with an integrated force measurement unit was constructed and validated. Subsequently, we investigated four different catheter models, each equipped with a unique measurement technology: Tacticath Quartz (Abbott), AcQBlate Force (Biotronik/Acutus), Stablepoint (Boston Scientific), and Smarttouch SF (Biosense Webster). For each model, the accuracy of three different catheters was measured within the range of 0-60 grams and at contact angles of 0°, 30°, 45°, 60°, and 90°. Results: In total, 6685 measurements were performed using 4x3 catheters (median of 568, IQR 511-606 measurements per catheter). Over the entire measurement-range, the force measured by the catheters deviated from the real force by the following absolute mean values: Tacticath 1.29g ±0.99g, AcQBlate Force 2.87g ±2.37g, Stablepoint 1.38g ±1.29g, and Smarttouch 2.26g ±2.70g. For some models, significant under- and overestimation of >10g were observed at higher forces. Mean absolute errors of all models across the range of 10-40g were <3g. Conclusion: Contact measured by force-sensing catheters is accurate with 1-3g deviation within the range of 10g to 40g. Significant errors can occur at higher forces with potential clinical consequences.