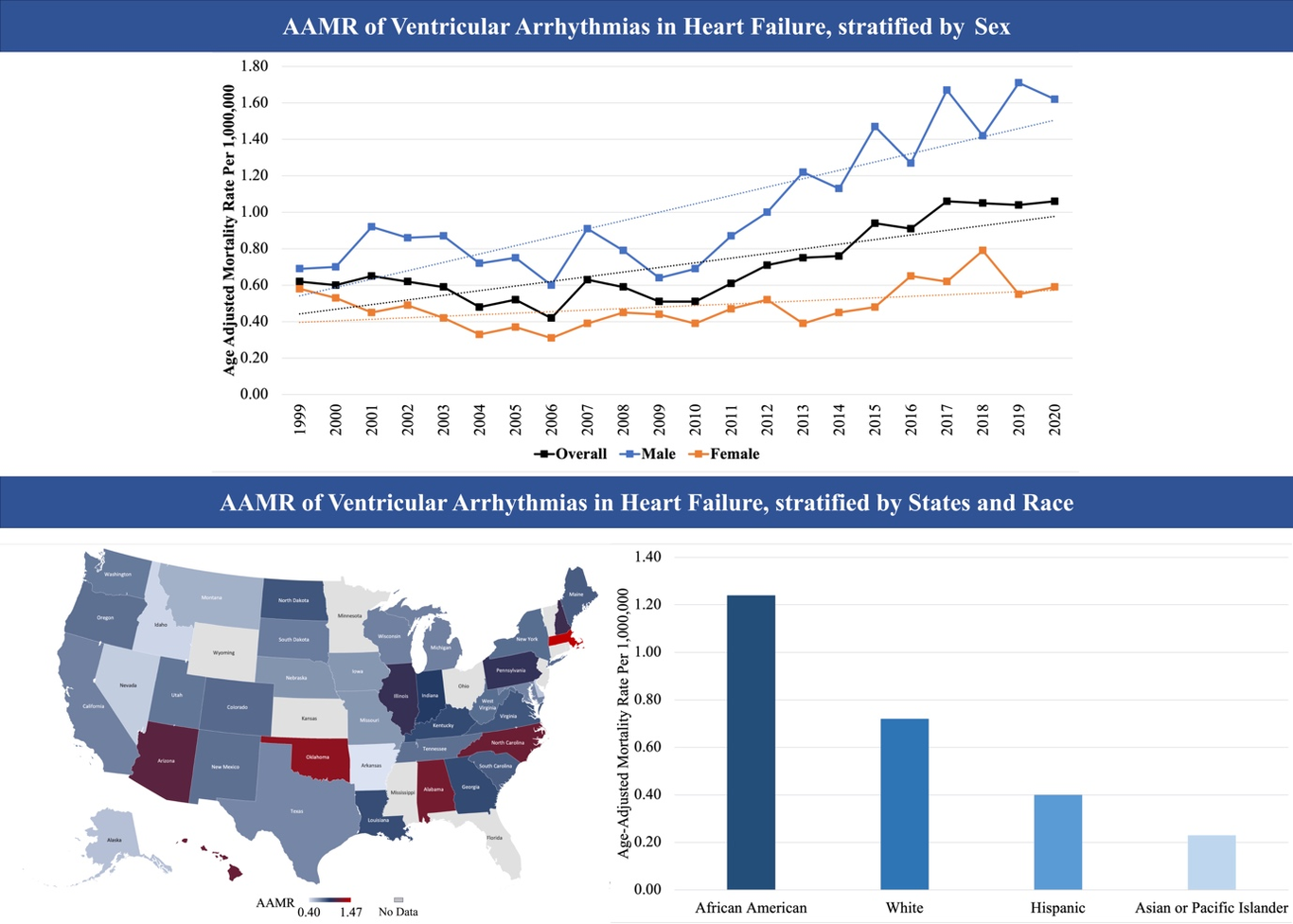
Ventricular Arrhythmia Mortality in Patients with Heart Failure in the United States: Are There Differences Based on Race and Geography?Min Choon Tan MD1,2, Yong Hao Yeo MBBS3, Boon Jian San MBBS4, Justin Z. Lee MD5, Kamala Tamirisa MD6, Yong-Mei Cha MD7, Luis R. Scott MD2, Dan Sorajja MD2, Andrea M. Russo MD81 Department of Internal Medicine, New York Medical College at Saint Michael’s Medical Center, Newark, NJ, USA2 Department of Cardiovascular Medicine, Mayo Clinic, Phoenix, AZ, USA3 Department of Internal Medicine/Pediatrics, William Beaumont University Hospital, Royal Oak, MI, USA4 AIMST University, Malaysia5 Department of Cardiovascular Medicine, Cleveland Clinic, Cleveland, OH, USA6 Texas Cardiac Arrhythmia, Dallas, TX, USA7 Department of Cardiovascular Medicine, Mayo Clinic, Rochester, MN, USA8 Department of Cardiovascular Medicine, Cooper University Health System/Cooper Medical School of Rowan University, Camden, NJ, USADisclosures: All authors have no relationships relevant to the contents of this paper to disclose.Ethical approval: Not requiredFunding: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectorsWord Count: 780Corresponding author:Andrea M. Russo MDDepartment of Cardiovascular Medicine,Cooper University Health System/Cooper Medical School of Rowan University1 Cooper Plaza,Camden, New Jersey [email protected] progression of heart failure (HF) is associated with detrimental myocardial structural changes, predisposing HF patients to an increased risk of ventricular arrhythmia (VA) events [1]. The evolving landscape in HF management as well as innovative approaches to VA like catheter ablation and neuromodulation, may impact morbidity and mortality. However, real-world data assessing the VA-related mortality trends among patients with HF remain scarce.The Centers for Disease Control and Prevention’s Wide-Ranging Online Data for EpidemiologicResearch (CDC WONDER) is a publicly available online database containing public health data, including mortality data. Death certificate data from CDC WONDER were analyzed from 1999 to2020 for VA-related mortality with comorbid HF among the U.S. population aged ≥ 25 years usingICD-10 codes. Ventricular arrhythmias included ventricular tachycardia (VT) (I47.2) and ventricularfibrillation (VF) (I49.0) as the underlying primary cause of death. Heart failure (I11.0, I13.0, I13.2,I50) was stated as a contributing cause of death. Age-adjusted mortality rates (AAMR) per 1,000,000individuals were calculated by standardizing VA-related mortality with comorbid HF to the 2000 U.S.census population. The trends were determined over time by estimating the annual percent change(APC) using the Joinpoint regression program. Given the deidentified and publicly available data,institutional review board approval was not required.Between 1999 and 2020, a total of 3,514 deaths related to VA with comorbid HF were identified.Overall, there was an increase in annual trends for the AAMR from 0.62 (95% CI, 0.50 - 0.73) in1999 to 1.06 (95% CI, 0.94 - 1.19) in 2020, with an APC of 3.39 (95% CI, 2.07, 4.73) (CentralIllustration) .When stratified by sex, cumulative AAMR was higher in males than females (1.09 [95% CI, 1.04-1.13] vs. 0.49 [95% CI, 0.47-0.52]). Both males and females had a similar increase in AAMR over the22 years; however, the AAPC was higher among males (4.30 [95% CI, 2.88-5.74] vs. 1.64 [95% CI,0.18-3.12]). When stratified by race, African American individuals had the highest AAMR (1.24 [95% CI, 1.14-1.35]), while the AAMR for White, Hispanic and Asian individuals were 0.72 (95% CI, 0.69-0.75), 0.40 (95% CI, 0.33-0.47), and 0.23 (95% CI, 0.16-0.32) respectively. The AAMR was higher in rural regions than in urban regions (0.81 [95% CI, 0.75-0.88] vs. 0.70 [95% CI, 0.68-0.73]). When AAMRs were compared between census regions of the U.S., the South region had the highest AAMR (0.86 [95% CI, 0.81-0.90]), followed by the Midwest (0.80 [95% CI, 0.75-0.85]), Northeast (0.62 [95%CI, 0.57-0.67]), and West region (0.56 [95% CI, 0.51-0.61]).This study provides crucial insight into VA-related mortality temporal trends and disparities among patients with comorbid HF. Despite advances in VA and HF management algorithms, our study revealed a 71% increase in AAMR in VA-related mortality with comorbid HF from 1999 to 2020. The observed growth in AAMR could be attributed to the rising use of cardiac implantable electronic devices, leading to increased recognition of VA as a terminal event [2]. Alternatively, more effective emergency medical services or greater availability of automatic external defibrillators may help to identify VT or VF as the initial rhythm recorded (rather than asystole or pulseless electrical activity). Our study raises the hypothesis that more diligent management of VA, including timely implantation of cardiac defibrillator devices and VT ablation could have an impact on this population.Our study demonstrates disparities in mortality trends, where American Africans and rural regionsrecorded higher AAMR. These may be potentially attributed to structural racism, conscious andunconscious biases, and the heightened socioeconomic challenges and access to medical care, presentin rural areas [3]. Limited or delayed access to complex tertiary care may impact mortality followingthe occurrence of sustained VA. Patients who live in rural or disadvantaged regions may not haveaccess to subspecialty referrals (such as electrophysiology or HF specialists) and may have delayed orlimited access to primary prevention therapies such as implantable cardioverter defibrillators orcardiac resynchronization therapy that may otherwise favorably influence outcomes. This highlightsthe need to address the potential causes of these inequalities and implement a focused policy thatincorporates the concept of social determinants of health to narrow the gap.There are several limitations in our study. First, due to the nature of death certificate data, an accurate assessment of the cause of death cannot be determined. Second, the database has no information at individual levels, such as comorbidity, ejection fraction, duration of diseases, and medical treatments, which are essential confounders for mortality.In conclusion, our study reveals an increase in VA-related mortality with comorbid HF, withdisparities seen in African Americans and rural regions. It underscores the pressing necessity for actions to facilitate the translation of treatment advancements into tangible improvements in mortality outcomes and healthcare inequalities.