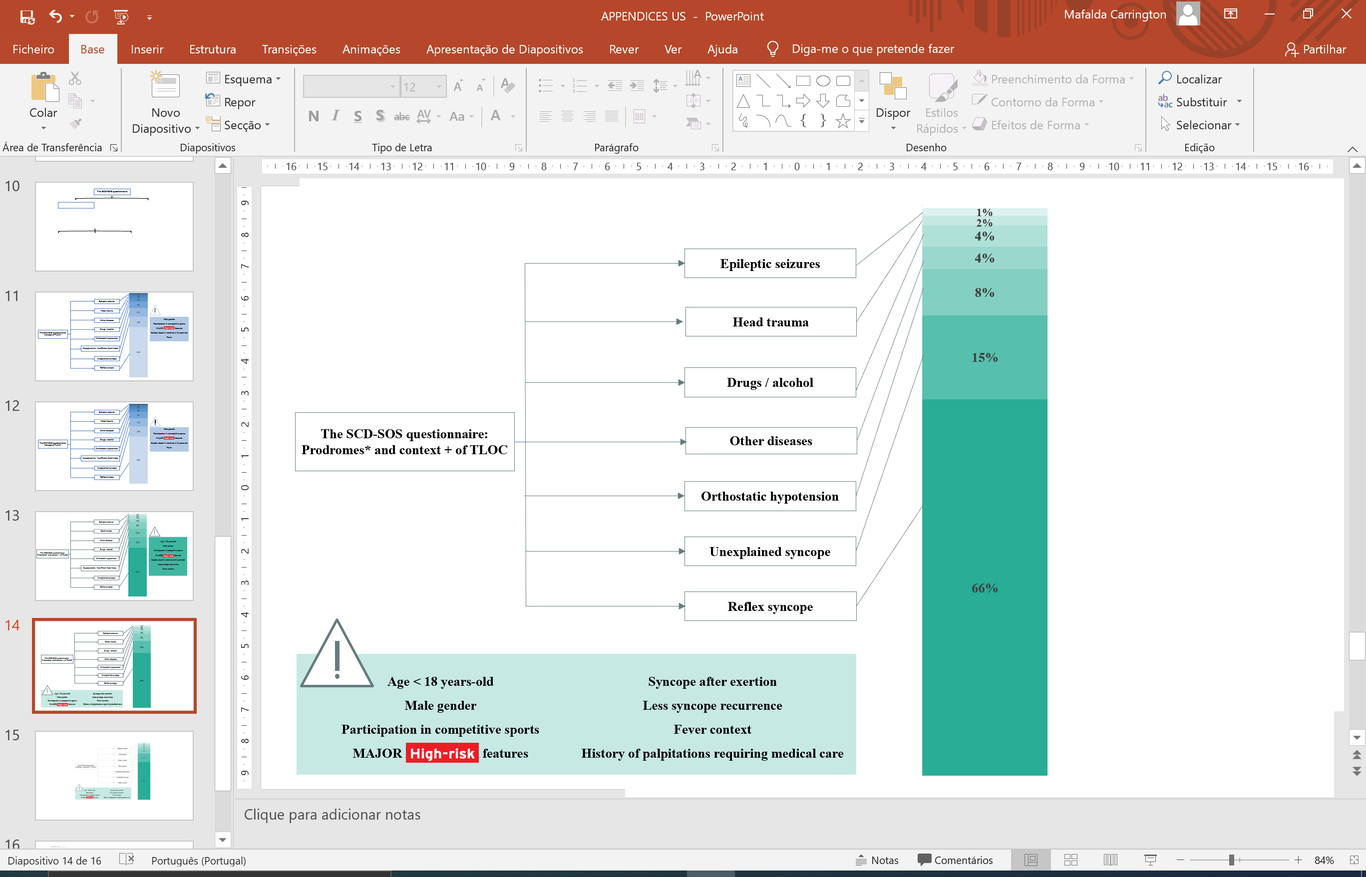
Introduction: The Sudden Cardiac Death-Screening of Risk FactOrS survey included a 12-lead ECG plus a digital-based questionnaire and aimed to screen for warning signs of diseases that may course with sudden cardiac death in children and young-adults. We aimed to estimate the prevalence of unexplained syncope (US) and characterize its high-risk features and predictors in this cohort. Methods and results: We determined the most probable etiology of the transient loss of consciousness (TLOC) episodes based on clinical criteria. US was an exclusion diagnosis and we analyzed its potential clinical and ECG predictors. Among 11,878 individuals, with a mean age of 21±6 (range 6-40) years-old, the cumulative incidence of TLOC was 26.5%, 76.2% corresponding to females. Reflex syncope was present in 61.0%, orthostatic hypotension in 7.9% and 12.6% of the individuals had US. Unexplained syncope was independently associated with age < 18 years-old (OR1.72; 95%CI 1.27-2.32,p<0.001), male gender (OR1.650; 95%CI 1.22-2.23,p=0.001), participation in competitive sports (OR1.64;95%CI 1.01-2.66,p=0.044), major syncope high-risk features (OR 2.61;95%CI 1.96-3.47,p<0.001), syncope after exertion (OR2.77;95%CI 1.80-4.27,p<0.001), fever context (OR9.58;95%CI 4.12-22.30,p<0.001), lower number of previous syncopal episodes (OR0.36;95%CI 0.37-0.48,p<0.001) and history of palpitations requiring medical care (OR1.98;95%CI 1.16-3.38,p=0.012). We found no ECG predictors of US in this population. Conclusions: The cumulative incidence of TLOC in children and young-adults is high and remains unexplained in an important proportion of individuals. We identified eight clinical characteristics that may be useful for the risk stratification of individuals evaluated in a non-acute setting.