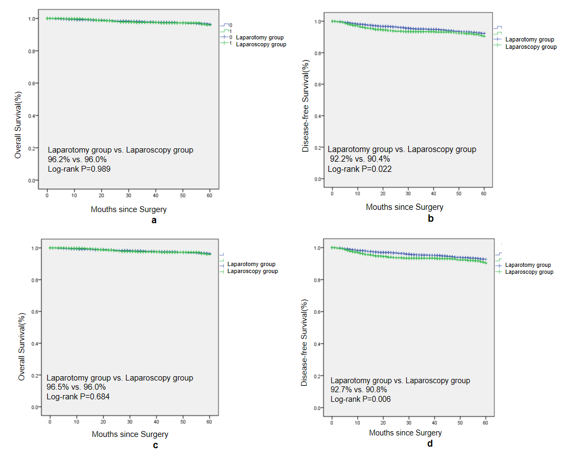
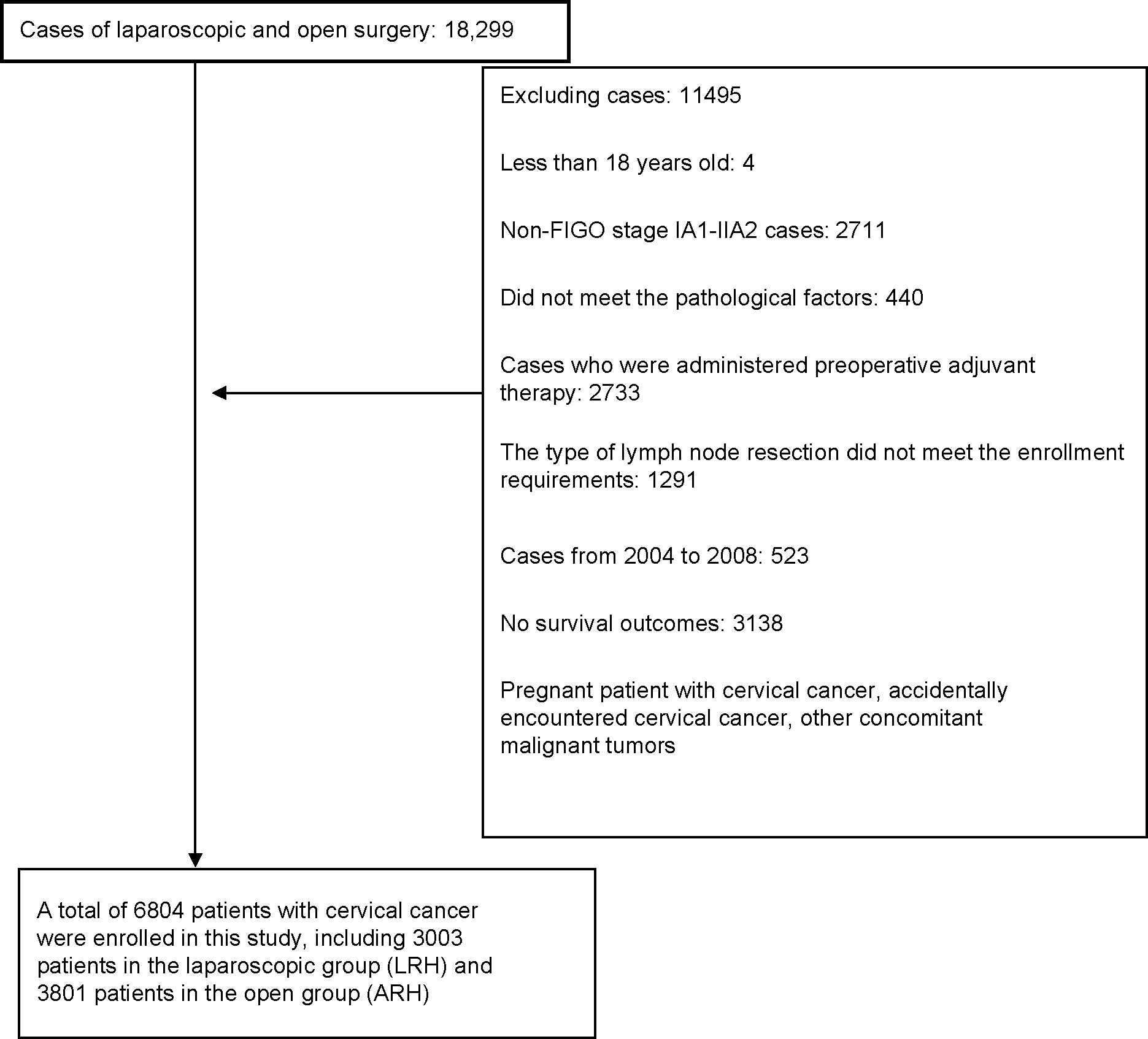
Objective Explore the difference of oncology outcome of laparotomy and laparoscopy in the new FIGO2018 stage of early cervical squamous cell carcinoma without any high risk pathological factors. Methods The 5-years OS and DFS of cervical squamous cell carcinoma undergoing laparotomy and laparoscopy from 2004 to 2018 were compared by the total study population and propensity score from China. Result There was no difference in 5-year OS between laparotomy (2,478 cases) and laparoscopy (1,504 cases), but the 5-year DFS of laparotomy was higher (92.2 %vs. 90.4%, P=0.022). Cox analysis showed that laparoscopy was not an independent risk factor for the death of cervical squamous cell carcinoma (OS: P=0.598), but it was an independent risk factor for the recurrence/death (HR = 1.468,95% CI 1.131 ~ 1.906, P=0.004). There was no difference in 5-year OS between laparotomy (2,391 cases) and laparoscopy (1,495 cases) after 1:2 PSM, but the 5-year DFS of laparotomy was higher (92.7% vs. 90.8%, P = 0.006), Cox analysis showed that laparoscopy was not an independent risk factor for the death of cervical squamous cell carcinoma (OS: P=0.521), but it was an independent risk factor for the recurrence/death (HR=1.512, 95%CI 1.151~1.971, P=0.002). Conclusion There is no difference in 5-year OS between these groups for early cervical squamous cell carcinoma in new stage of FIGO2018 without any high-risk pathological factors, the 5-year DFS of laparotomy is higher than that of laparoscopy group, and laparoscopy is an independent risk factor for recurrence/death, so laparoscopy has a higher risk of recurrence.