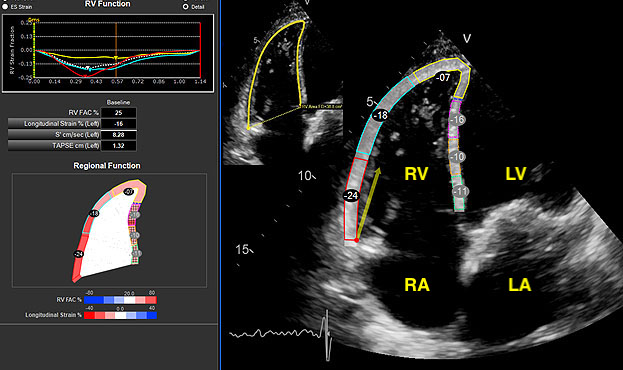
Background: Transapical transcatheter mitral valve implantation (TMVI) may be a therapeutic option for patients with severe mitral regurgitation (MR) excluded from cardiac surgery due to excessive risk. Common reasons for exclusion from surgery are pulmonary hypertension and right ventricular (RV) dysfunction. The effect of TMVI on RV function has not previously been well-characterized. Objectives: The aim of this study was to examine the procedural and 3-month impact of TMVI on RV hemodynamics and remodeling. Methods: This was a multi-center, retrospective, observational cohort study of patients with >3+MR undergoing TMVI. Pre- and post-TMVI hemodynamics were assessed with right heart catheterization. RV remodeling was assessed at baseline, pre-discharge and at 3-months by echocardiography. Results: Forty-six patients (age 72±9 years; 34 men) with ≥3+MR underwent TMVI over a 5-year period. Successful device implantation was achieved in all patients with abolition of MR (p<0.001) and reduction in left-ventricular end-diastolic volume (p=0.001). RV stroke work index increased intra-operatively (7±4g/m/beat/m² vs 11±5g/m/beat/m²; p<0.001). At 3-months there were reductions in severity of tricuspid regurgitation (TR) (p<0.001) and pulmonary artery systolic pressure (PASP) (49±16mmHg vs 36±12mmHg; p<0.001), and improvements in RV fractional area change (28±7% vs 34±9%, p<0.001), tricuspid annular plane systolic excursion (TAPSE) (1.0±0.3 vs 1.5±0.5cm, p=0.03), and RV free wall longitudinal strain (-14.2±5.0 vs -17.6±7.3, p=0.05). Conclusions: Transapical TMVI results in significant improvement of RV function that is sustained to 3 months as evidenced by reductions in TR severity and PASP, and improvements in RV fractional area change, TAPSE, and RV free wall longitudinal strain.