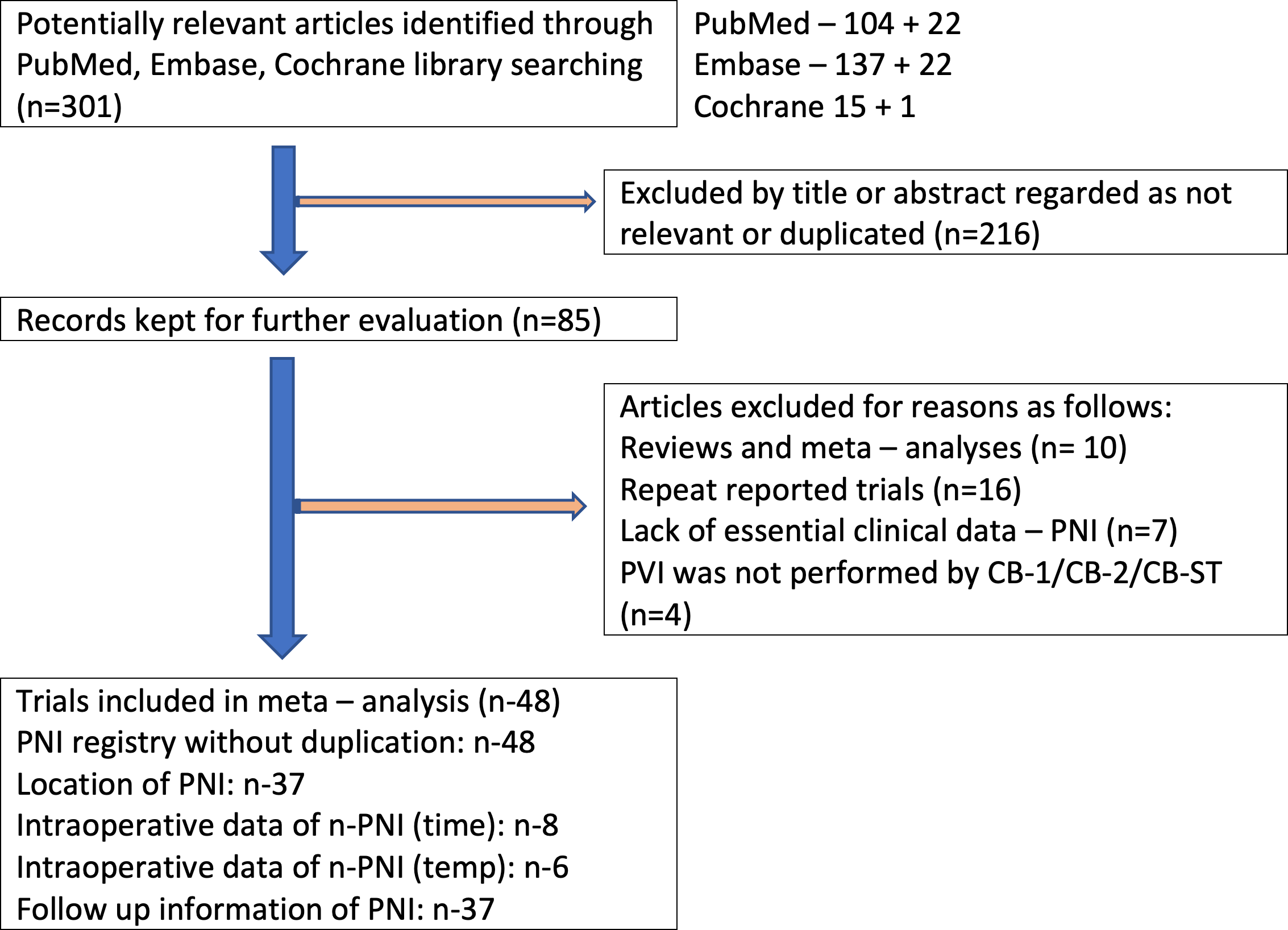
Background: The right phrenic nerve is vulnerable to injury (rPNI) during cryoballoon ablation (CBA) isolation of the right pulmonary veins. The complication can be transient or persistent. The reported incidence of rPNI fluctuates from 4.73% to 24.7% depending on changes over time, CBA-generation, and selected protective methods. Methods: Through September 2019, a database search was performed on MEDLINE, EMBASE, and Cochrane Database. In the selected articles, the references were also extensively searched. The study provides a comprehensive meta-analysis of the overall prevalence of rPNI, assesses the transient to persistent PNI-ratio, the outcome of using compound motor action potentials (CMAP), and estimated average time to nerve recovery. Results: From 2008 to 2019, 10,341 records from 48 trials were included. Out of 783 eighty- PNI (7.7%), 589 (5.7%) were transient, and 194 (1.9%) were persistent. CMAP caused a significant reduction in the risk of persistent PNI from 2.3% to 1.1% (p = 0.05; odds ratio [OR] 2.13) in all CBA groups. The mean time to rPNI recovery extended beyond the hospital discharge was significantly shorter in CMAP group at three months on average versus non CMAP at six months (p = 0.012). CMAP (in contrast to non-CMAP procedures) detects PNI earlier from 4 to 16 sec (p < 0.05; I2 = 74.53%) and 3 to 9º (p < 0.05; I2 = 97.24%) earlier. Conclusions: rPNI extending beyond hospitalization is a relatively rare complication. CMAP use causes a significant decrease in the risk of prolonged injury and shortens the time to recovery