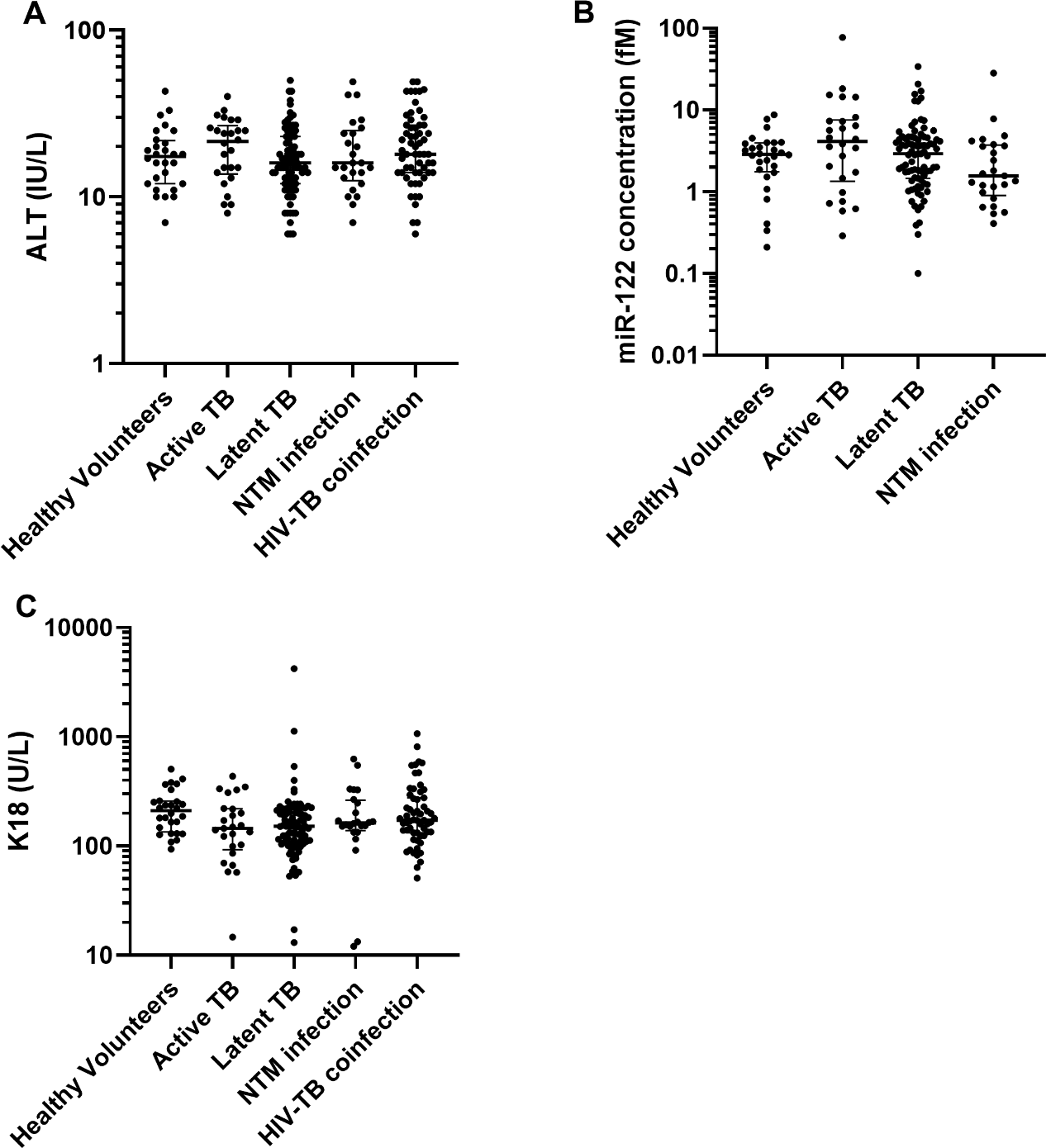
Aim Patients on anti-tuberculosis (anti-TB) therapy are at risk of drug-induced liver injury (DILI). MicroRNA-122 (miR-122) and cytokeratin-18 (K18) are exploratory DILI biomarkers. To explore their utility in this global context, circulating miR-122 and K18 concentrations were measured in UK and Ugandan populations on anti-TB therapy for mycobacterial infection. Methods European patients receiving anti-TB therapy were recruited at the Royal Infirmary of Edinburgh, UK (ALISTER-ClinicalTrials.gov Identifier: NCT03211208). African patients with HIV-TB coinfection, receiving anti-TB and anti-retroviral therapy (ART), were recruited at the Infectious Diseases Institute, Kampala, Uganda (SAEFRIF-NCT03982277). Serial blood samples, demographic and clinical data were collected. MiR-122 was quantified using PCR. K18 was quantified using the M65 ELISA. Results The study had 235 participants (healthy volunteers (n=28); ALISTER: active TB (n=30), latent TB (n=88), non-tuberculous mycobacterial infection (n=25); SAEFRIF: HIV-TB coinfection (n=64)). In the absence of DILI, there was no difference in miR-122 and K18 across the groups. Both miR-122 and K18 correlated with alanine transaminase activity (ALT) (miR-122: r=0.52, 95%CI=0.42-0.61, P<0.0001. K18: r=0.42, 95%CI=0.34-0.49, P<0.0001). There were two DILI cases: baseline ALT was 18 and 28 IU/L, peak ALT 431 and 194 IU/L; baseline K18 58 and 219 U/L, peak K18 1247 and 3490 U/L; baseline miR-122 4 and 17 fM, peak miR-122 60 and 336 fM, respectively. Conclusion In European and African patients treated with anti-TB therapy miR-122 and K18 correlated with ALT and increased with DILI. Further work should determine the diagnostic and prognostic utility of miR-122 and K18 in this global context-of-use.