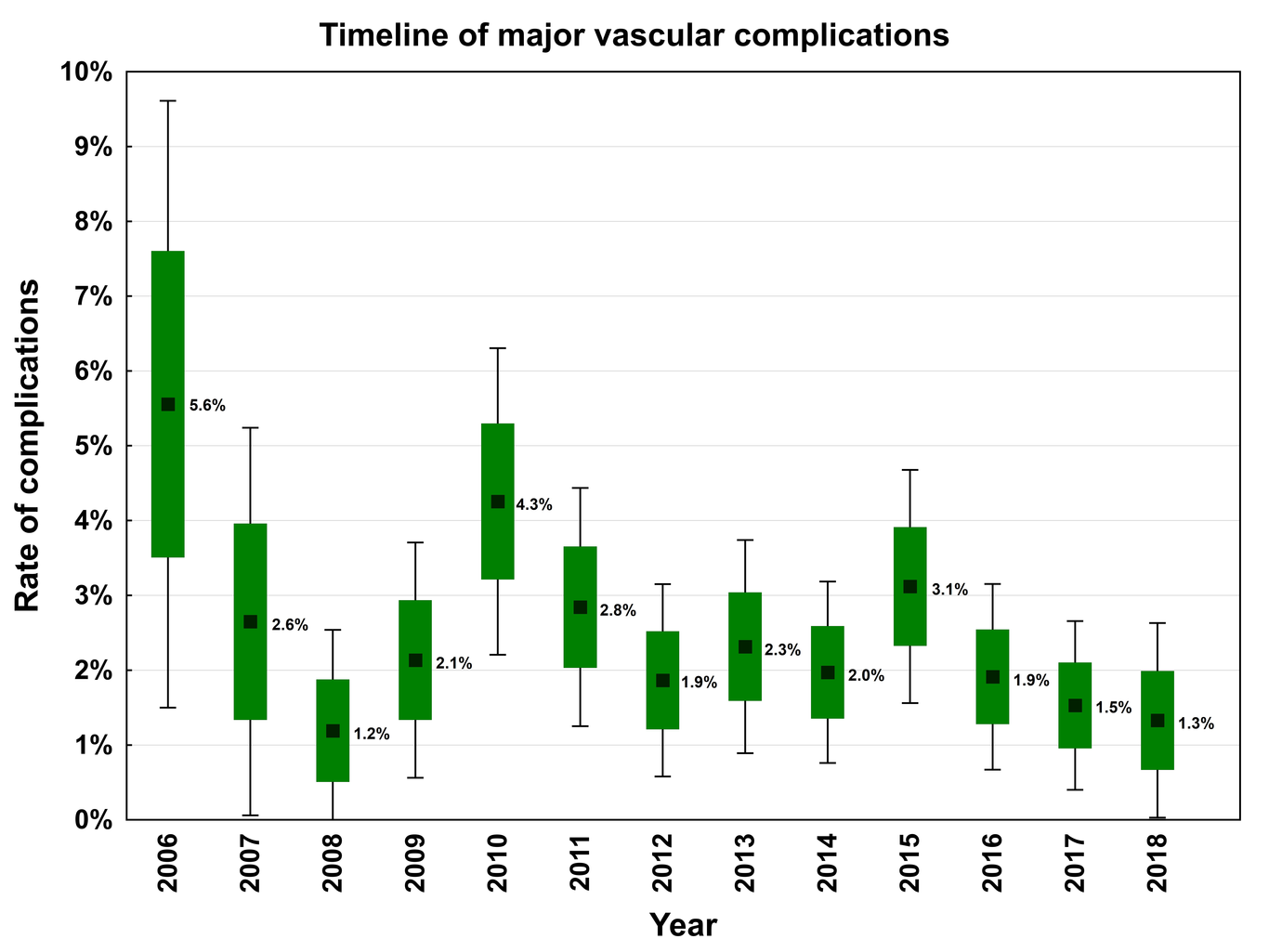
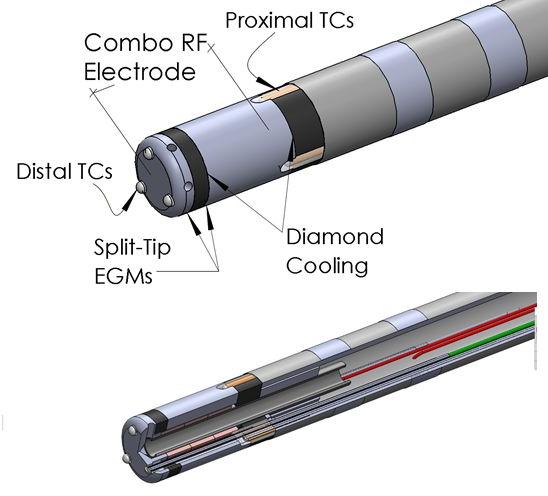
Aims: Saline-irrigated radiofrequency ablation (RFA) for atrial fibrillation (AF) is limited by the absence of reliable thermal feedback limiting the utility of temperature monitoring for power titration. The DiamondTemp (DT) ablation catheter allow efficient temperature-controlled irrigated ablation. We sought to assess the 1-year clinical safety and efficacy of the DT catheter in treating drug-refractory paroxysmal AF. Methods and results: The TRAC-AF trial (NCT02821351) is a prospective, multi-center (n=4), single-arm study that enrolled patients with symptomatic, drug-refractory paroxysmal AF. Using the DT catheter, point-by-point ablation was performed around all pulmonary veins (PVs) to achieve PV isolation (PVI). Ablation was performed in a temperature-control mode (60oC, max 50 W) until the split-tip EGM amplitude decreased by ≤75%. The primary efficacy endpoints included acute procedural success and freedom from AF at 12 months. A total of 62 patients (age 60.3 ± 11.4 years; 60% male) were evaluated after AF ablation using the DT catheter. The mean fluoroscopy and RF ablation times were 9.4±6.4 min and 19.8±8.6 min, respectively. Acute isolation of all PVs was achieved in 100% of patients. There were no steam pops and there were not seen any char or caugulum on the catheter tip after ablation. There were very few serious procedure/device-related adverse events including a single case of cardiac tamponade (1.6%). At 1 year, the freedom from AF was 74.2%. Conclusion: This first in man series demonstrates that temperature-controlled irrigated RFA with the DT catheter is efficient, safe, and effective in the treatment of paroxysmal AF.