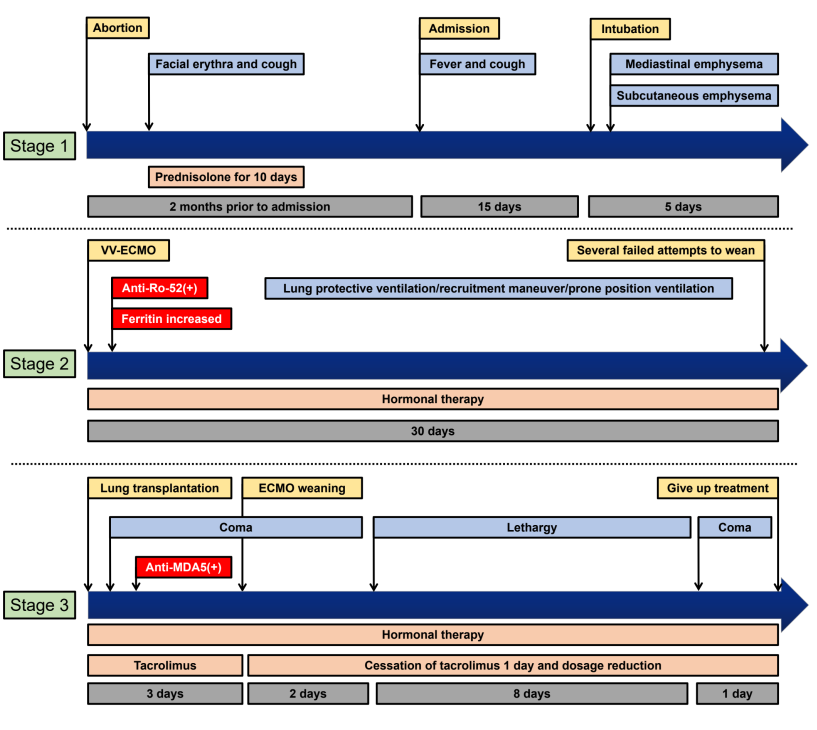
A 36-year-old woman was referred to a local hospital with cough and fever. She had a history of facial erythema and cough that began 2 months ago. Her status developed into rapid progressive interstitial lung disease (RP-ILD) with mediastinal emphysema and subcutaneous emphysema after admission, and venovenous extracorporeal membrane oxygenation (V-V ECMO) was initiated. After several failed attempts to wean the patient from ECMO, a decision was made to place the patient on the lung transplant waitlist. She underwent a double lung transplant on ECMO day 31 and received tacrolimus as an immunosuppressive regimen. The patient presented with positive anti-MDA5 and anti-Ro-52 antibodies and a high ferritin level, all of which indicated the presence of clinically amyopathic dermatomyositis (CADM). The patient was weaned from ECMO at 3 days after transplantation, but the patient’s state of consciousness deteriorated, and head CT was considered for posterior reversible encephalopathy syndrome (PRES). After the temporary cessation of calcineurin inhibitors and a dosage reduction, the patient’s state of consciousness returned to normal. Because of another disturbance of consciousness, the patient declined further treatment and was discharged 14 days after transplantation.