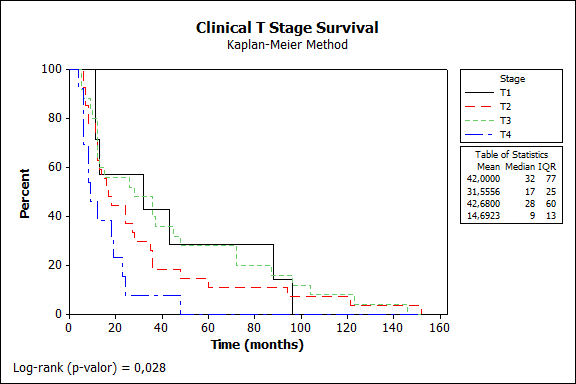
Objective: To investigate the prognostic factors to developing parotid and neck metastasis in locally advanced and relapsed cutaneous squamous cell carcinoma (CSCC) of the head and neck region. Study Design: Retrospective cohort study. Setting: Single-center study enrolling consecutive patients with advanced CSCC from 2009 to 2019. Subjects and Methods: Seventy-four cases were identified. Study variables demographic data, clinical skin tumor stage, neck stage, parotid stage (P stage), surgical treatment features, and parotid, regional, and distant metastases. Survival measures: overall survival (OS) and disease-specific survival (DSS). Results: The study group included 72.9% men (median age, 67 years); 67.5% showed T2/T3 tumors, 90.5% comorbidities, 20.2% immunosuppressed, with median follow-up: 35.8 months. The most frequent skin primary were auricular and eyelid regions, 75% underwent primary resection with flap reconstruction. Parotid metastasis was present in 50%, 32.4% showing parotid extracapsular spread, multivariate analysis found OR=37.6 of positive parotid metastasis evolve into positive neck metastasis, p=0.001. Occult neck metastasis, neck metastasis, and neck extracapsular spread were observed in 13.5%, 51.3%, and 37.8%, respectively. Kaplan-Meier survival: Clinical T4 and T1, p=0.028, P1 stage: 30% and 5% survival at 5 and 10 years, P3 stage: 0%, p=0.016; OS and DSS showed negative survival for the parotid metastasis group, p=0.0283. Conclusion: Our outcomes support a surgically aggressive approach for locally advanced and relapsed CSCC, with partial parotidectomy for P0, total parotidectomy for P1-3, selective I-III neck dissection for all patients and adjuvant radiochemotherapy to appropriately treat patients with advanced CSCC of the head and neck region.