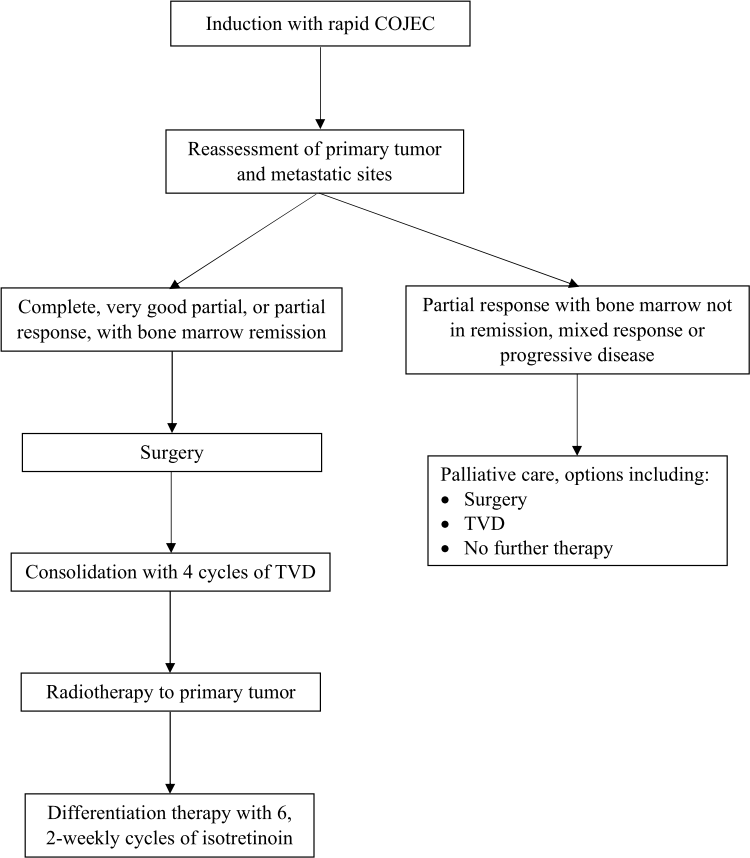
Background: The majority of patients with high-risk neuroblastoma (HR-NB) in low- and middle-income countries (LMIC) do not have access to autologous stem cell transplant (ASCT) and dinutuximab. Consolidation with non-myeloablative chemotherapy is not well-defined, and the outcomes are variable. We report a single-center outcome of patients with HR-NB, treated with non-myeloablative consolidation. A tabulated compilation of similar reports is included. Procedure: A retrospective chart review of patients with HR-NB was performed from January 2009 till June 2016. Patients were treated on the backbone of HR-NBL1/SIOPEN protocol. Treatment included induction with rapid-COJEC, surgery, consolidation, radiotherapy to the primary tumor, and differentiation therapy with isotretinoin. Consolidation included 4 cycles of topotecan, vincristine, and doxorubicin (TVD) instead of ASCT. Infusion of vincristine and doxorubicin were modified for ease and to enable administration in daycare. Results: Over 7-½ years, 28 patients with HR-NB were treated. Two (7%) patients had therapy-related mortality. A relapse or disease progression occurred in 11 (39%) patients at a median duration of 17 months (IQR: 5, 18). Treatment abandonment was observed in 4 (14%) patients. The 4-year event-free survival was 29.3%. The median follow up of disease-free patients is 49 months (IQR: 45, 79). Patients with relapse were not treated further. Conclusions: A 4-year EFS of 29.3% was observed when 4-cycles of TVD were administered instead of ASCT in patients with HR-NB. The study and the review will aid stakeholders in LMIC for decision-making while considering the options of treatment for HR-NB if access to ACST and dinutuximab is lacking.