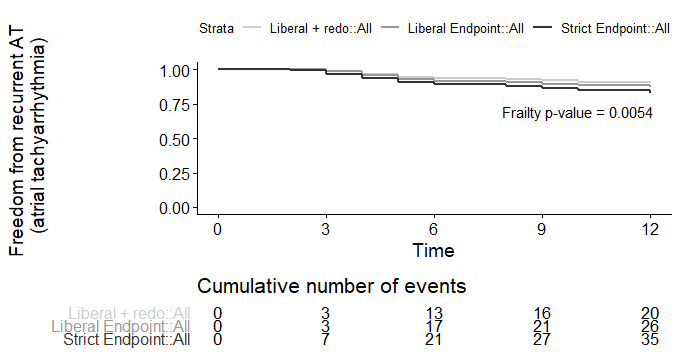
INTRODUCTION: Different endpoint criteria, different durations of follow up and the completeness of follow up can dramatically affect the perceived benefits of Atrial Fibrillation (AF) ablation. METHODS: We defined three endpoints for recurrence of AF post ablation in a cohort of 200 patients with symptomatic AF, refractory to antiarrhythmic drugs (AADs). A “Strict Endpoint” where patients were considered to have a recurrence with any symptomatic or documented recurrence for ≥30 seconds with no blanking period, and off their AADs, a “Liberal Endpoint” where only documented recurrences after the blanking period, either on or off AADs were counted, and “Liberal Endpoint + Redo” which was the same as the Liberal endpoint but allowing for 1 redo ablation or 1 cardioversion (DCCV) during follow up. We also surveyed 50 patients on the waiting list for an AF ablation and asked them key questions regarding what they would consider to be a successful result for them. RESULTS: Freedom from recurrence of atrial tachyarrhythmias (AT) at 5 years was 62% for the strict endpoint, 73% for the liberal endpoint, and 80% for the liberal endpoint + redo group (p<0.001). Of the 50 patients surveyed awaiting AF ablation, 70% said they would still consider the procedure a success if it required one repeat ablation or one DCCV (p=0.004), and 76% would be accepting of one or two recurrences during follow-up (p<0.001). CONCLUSION: In this study the most important predictor of AT recurrence following AF ablation was the criteria used to define recurrence.