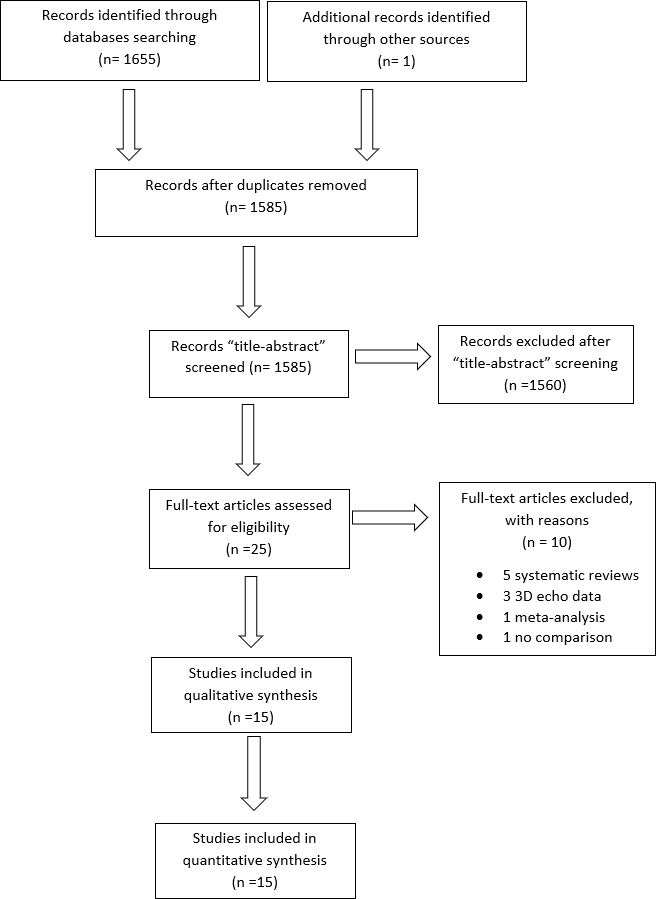
Background: Right ventricular failure (RVF) following Left Ventricular Assist Device (LVAD) implantation is associated with worse outcomes. Prediction and early identification of RVF with speckle-tracking echocardiography (STE) has been proposed. Methods: We queried multiple databases for articles reporting on pre-operative/intraoperative global longitudinal strain (GLS) and free-wall strain (FWS) in LVAD recipients. We performed a systematic review and meta-analysis of published literature. The standard mean difference (SMD) in GLS and FWS in patients with and without RVF postoperatively was pooled using random effects model. Results: Fifteen studies, with a total of 967 LVAD recipients were included. There was statistically significant difference in GLS among patients who did and did not develop RVF; SMD= -3.09 (95% CI: -4.62 to -1.57; p-value <0.0001). There was significant difference in FWS between two groups; SMD: -2.75 (95% CI: -3.72 to -1.79; p-value <0.0001). Upon subgroup analysis of imaging modality, transthoracic echocardiography (TTE)-derived GLS and FWS remained predictive for RVF with SMD of -3.97 (95% CI: -5.40 to -2.54; p-value <0.001) and -3.05 (95% CI: -4.11 to -1.99; p-value <0.001), respectively. However, there was no significant difference between RVF and non-RVF groups upon using transesophageal echocardiography (TEE) to assess GLS and FWS. Conclusion: GLS and FWS assessment of the RV by STE is a useful tool to predict postoperative RVF in LVAD recipients. While the predictive role of TTE was robust, the TEE-derived measures seemed to be less predictive. Future studies need to specify the strain cut-off value that can predict the adverse outcome of RVF