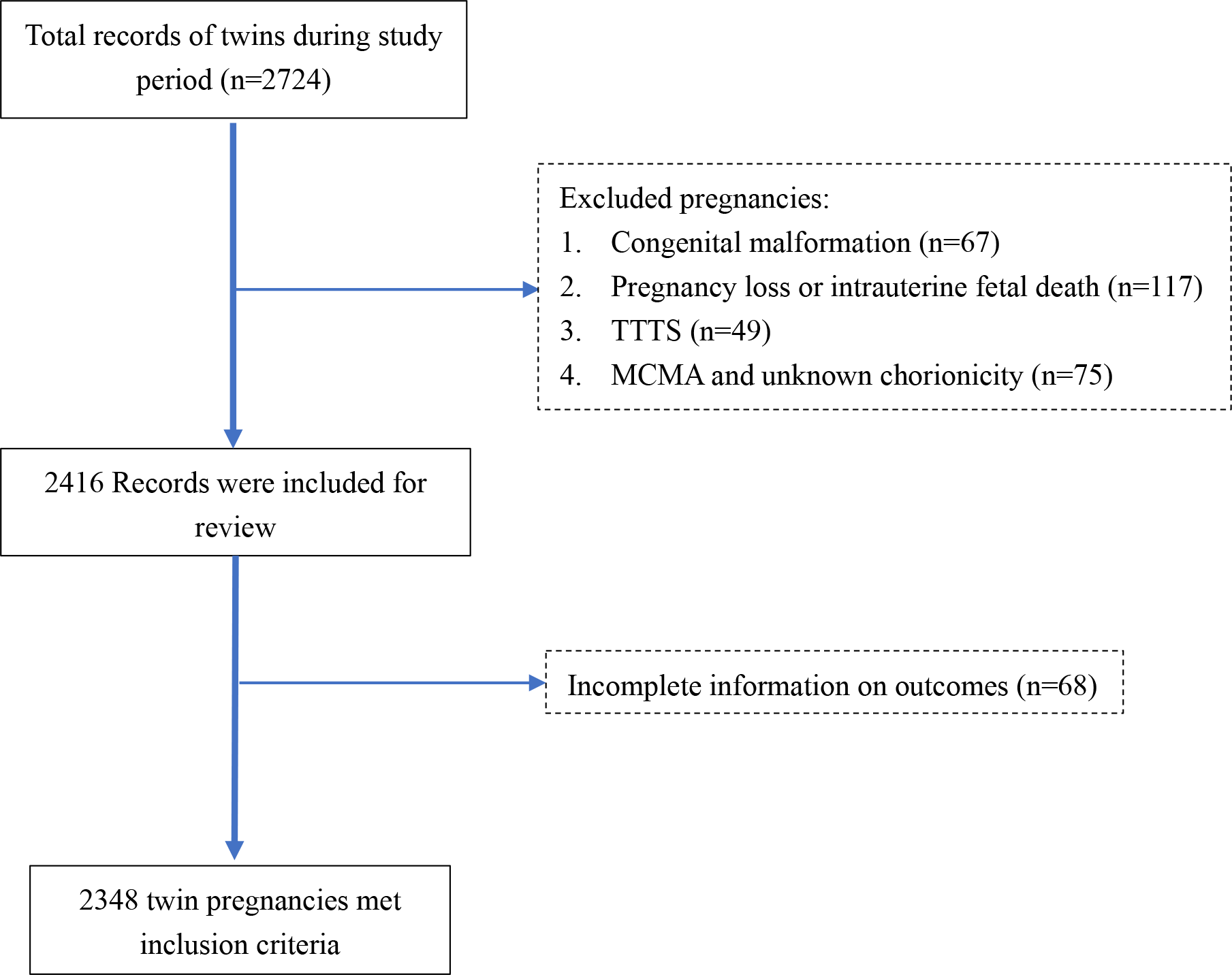
Objective: To evaluate the thresholds of BWD for predicting early neonatal outcomes and assess the predictive accuracy of BWD. Design: Retrospective cohort study. Setting: Single Chinese University Hospital. Population: All women with liveborn twins at gestational age of ≥ 26 weeks. Methods: Multivariable logistic regression analyses of association between neonatal outcomes and BWD with different thresholds (≥15.0%, ≥20.0%, ≥25% and ≥30%). Generalized estimated equation (GEE) models to address inter-twin correlation. Restrictive cubic spline (RCS) models to draw the dose-response relationship. Clustered receiver operating characteristic (ROC) curve analysis to assess the predictive accuracy. Main outcomes: NICU admission, neonatal respiratory distress syndrome (NRDS), ventilator support and composite outcome including major morbidity and neonatal death. Results Among 2348 twin pairs, BWD were at significantly increased risks of NICU admission, irrespective of the thresholds. The risks of NRDS, ventilator support and composite outcome were significantly higher when a threshold of ≥20% or above was chosen. The dose-response relationship showed non-linear growth in risk of adverse neonatal outcomes with the increasing BWD. ROC analyses showed a low significant AUROC of 0.569 (95% CI: 0.526-0.612) for predicting NICU admission but no significant AUROC for predicting other outcomes. A BWD of ≥30% provided a moderate increase in the likelihood of NICU admission [positive likelihood ratio (LR+) =5.77]. Conclusions BWD is independently associated with adverse neonatal outcomes. Regardless of this association, BWD could not serve as a single predictor for neonatal outcomes. A cut-off of 30% is more practical for risk stratification among twin gestations.