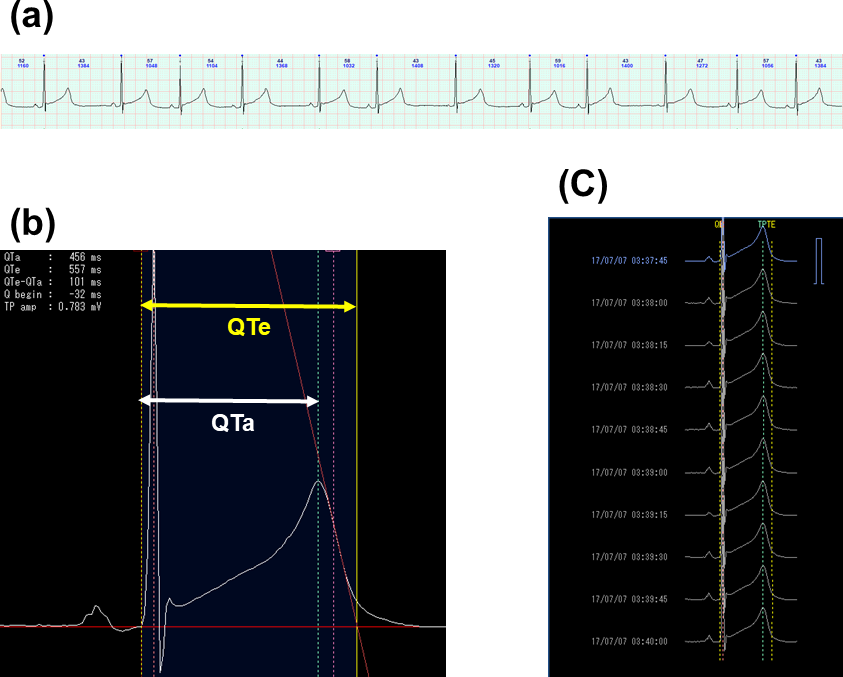
Background The clinical course and therapeutic strategies in the congenital long QT syndrome (LQTS) are genotype-specific. However, accurate estimation of LQTS-genotype is often difficult from the standard 12-lead ECG. Objectives This study aims to evaluate the utility of QT/RR slope analysis by the 24-hour Holter monitoring for differential diagnosis of LQTS-genotype between LQT1 and LQT2. Methods This cross-sectional study enrolled 54 genetically identified LQTS patients (29 LQT1 and 25 LQT2) recruited from 3 medical institutions. The QT-apex (QTa) interval and the QT-end (QTe) interval at each 15-second were plotted against the R-R intervals and the linear regression (QTa/RR and QTe/RR slopes, respectively) were calculated from the entire 24-hour and separately during the day or night-time periods of the Holter recordings. Results The QTe/RR and QTa/RR slopes at the entire 24-hour were significantly steeper in LQT2 compared to those in LQT1 patients (0.262 +/- 0.063 vs 0.204 +/- 0.055, P = 0.0007; 0.233 +/- 0.052 vs 0.181 +/- 0.040, P = 0.0002, respectively). The QTe interval was significantly longer, QTe/RR and QTa/RR slopes at daytime were significantly steeper in LQT2 than in LQT1 patients. The receiver operating curve analysis revealed that the QTa/RR slope of 0.211 at the entire 24-hour Holter was the best cut-off value for differential diagnosis between LQT1 and LQT2 (sensitivity: 80.0%, specificity: 75.0% and area under curve: 0.804 [95%CI = 0.68-0.93]). Conclusion The continuous 24-hour QT/RR analysis using the Holter monitoring may be useful to predict the genotype of congenital LQTS, particularly for LQT1 and LQT2.