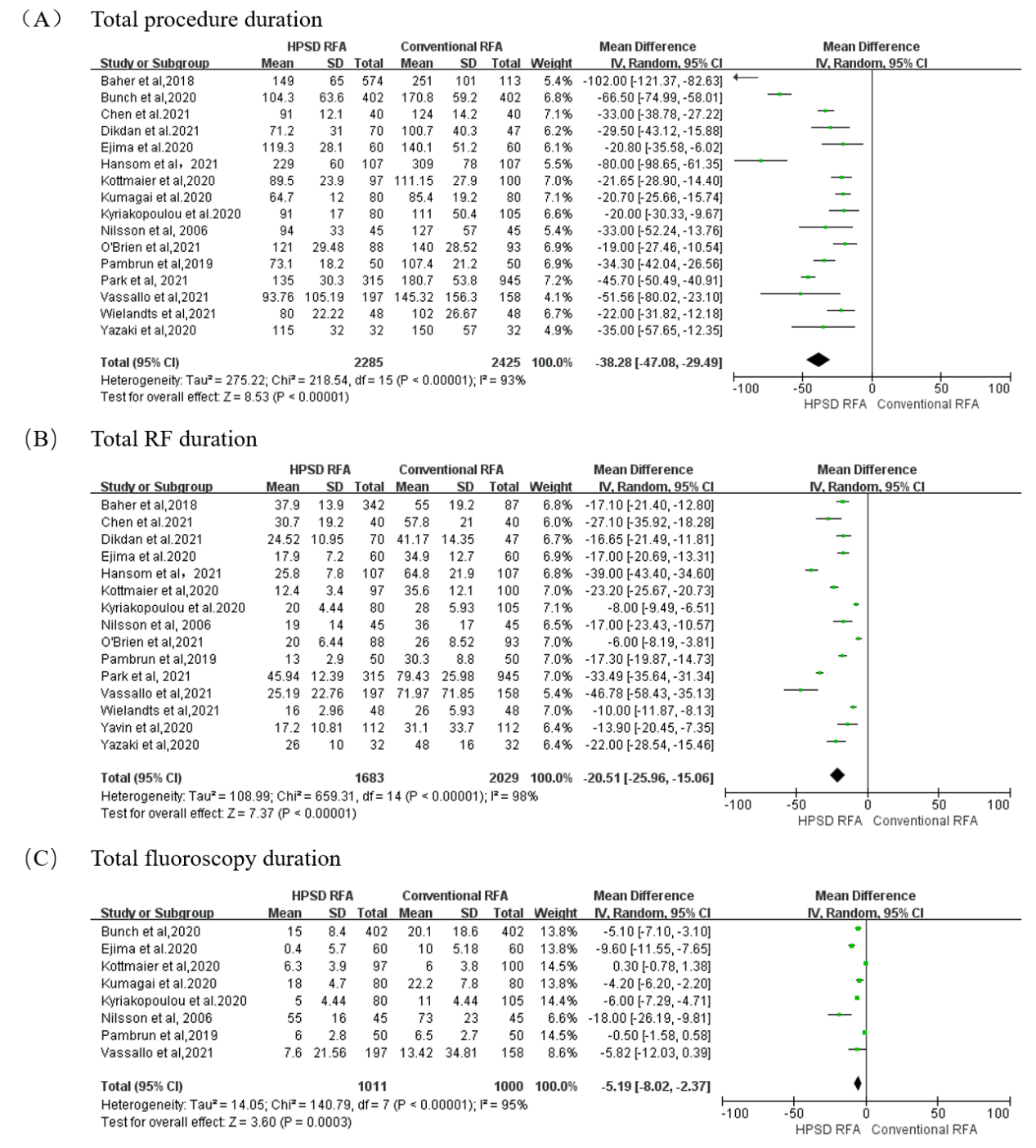
Aims: We aimed to further evaluate the effectiveness and safety between high-power short-duration (HPSD) radiofrequency ablation (RFA) and conventional RFA in patients with atrial fibrillation (AF). Methods: Studies comparing HPSD and conventional applications from inception through December 2021 were searched on Pubmed, Medline, Cochrane and Clinicaltrials.gov. Results: The meta-analysis included seventeen studies with a total of 4934 patients. HPSD group decreased procedure duration [mean difference (MD) -38.28 min, 95% confidence interval (CI) -47.08 to -29.49, P<0.001], RF duration (MD -20.51 min, 95% CI -25.96 to -15.06, P<0.001) and fluoroscopy duration (MD -5.19 min, 95% CI -8.02 to -2.37, P<0.001), while improving the rates of first-pass isolation [Odds Ratio (OR) 8.92, 95% CI 2.40-33.09, P=0.009]. Compared with conventional group, freedom from atrial arrhythmia at 1-year-followup was higher in the HPSD group with a power setting of 40-50W (OR 1.93, 95% CI 1.27-2.91, P=0.002), nevertheless, two groups had similar effectiveness with a power setting of 50W in the HPSD RFA (OR 1.10, 95% CI 0.83-1.46, P=0.52). Acute pulmonary vein reconnection (P<0.001) was significantly lower in the HPSD group. There was no difference in complications between the two groups (P=0.71). Conclusion: HPSD RFA was associated with shorter procedure duration, higher freedom from atrial arrhythmia and comparable safety when compared with conventional RFA.