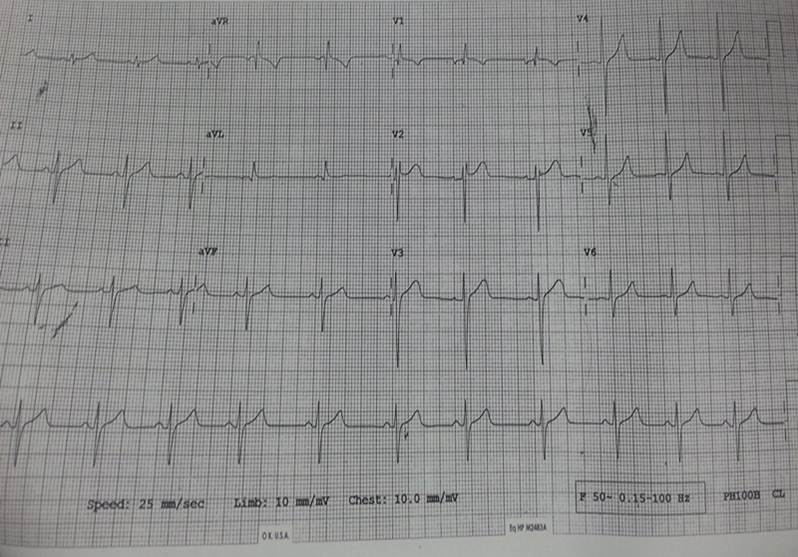
A 1 year female child, first in birth order, born term out of nonconsanguineous marriage through normal vaginal delivery and had uneventful postnatal period. She had history of recurrent episodes of tachypnea. On examination patient was hemodynamically stable, afebrile with heart rate of 84 beats/minutes in sinus rhythm, blood pressure of 112/65mm Hg with Spo2 of 99%. On cardiac examination there were normal findings except soft systolic murmur. Echocardiography (echo) revealed a single solid mass arising from papillary muscle extending into left ventricular (LV) posterior wall upto crux of heart measuring 2.7x2.7cms likely of Ventricular Fibroma. Cardiac MRI (CMR) revealed well defined mass lesion of 3.9x3.8 cm arising from posterior wall of left ventricle extending posteriorly with exophytic component showing homogenous delayed enhancement confirming our diagnosis of ventricular fibroma. Her Holter showed intermittent episodes of non-sustained broad complex tachycardia suggestive of Ventricular Tachycardia. She was then discharged on oral Amiodarone and Propanolol and kept on continuous follow up. At 2 years of age she was readmitted with history of palpitation and ECG done showed ventricular tachycardia. She was kept on oral Amiodarone and Propanolol with continuous monitoring. Echo done similar findings but the mass was gradually increasing in size(37x35cms). Holter and ECG showed frequent episodes of wide QRS tachycardia most likely VT,??SVT with aberrancy. Hemodynamics of the child were maintained during the episodic cardiac arrhythmias. CMR was repeated which showed increase in well defined mass measuring 43x42cms arising from mid basal posterior inferior wall of LV extending posteriorly with exophytic component . PET CT scan was done showed non FDG avid nodular lesion in relation with left ventricle suggestive of Fibroma. Her Thyroid profile is being monitored and is within normal range. Sotalol has been introduced in the management of the child and Amiodarone was withdrawn .It demonstrated transient episodes of tachycardia which are non sustained. Child is being kept under regular follow upPrimary cardiac tumors are rare with incidence of 0.03-0.32%.1Cardiac fibroma predominantly affects children and is second most common benign tumor. The most common site is left ventricle(57%) followed by right ventricle(27.5%) and interventricular septum(17%).1Although cardiac fibromas are asymptomatic some may present with serious complications like arrhythmias and intracavitary obstruction. Ventricular tachycardia have been reported in few cases of cardiac fibroma2,3which was also found in our case.Our case was collectively discussed with pediatric cardiothoracic team, radiology and electrophysiology meet. Surgery was deferred keeping in view the extensive involvement of left ventricle which hindered the cleavage plane. Few literatures recommend strategy of postponing surgery and adequate management of ventricular tachycardia for tumors not amenable to resection which would increase the chances of successful surgical outcome later.2REFERENCES:1.Furqan A.Rajput,Faten Limaiem.Cardiac Fibroma.[Updated 2020 Apr 29].In:StatPearls[Internet].Treasure Island(FL):StatPearls Publishing;2020 Jan-.2.Alyssa L .Ritter,Eric J.Granquist,V.Ramesh Iyer,Kosuke Izumi.Cardiac Fibroma with ventricular Tachycardia:An unusual Clinical Presentation of Nevoid Basal Cell Carcinoma Syndrome.Mol Syndromol 2018;9:219-2233.Alice Horovitz,Irene E.van Geldorp,Francis Roubertie,Jean-Benoit Thambo.Large Right Ventricular Fibroma in a 6 month-old infant.Pediatr Cardiol(2012) 33:1458-1460LEGENDSFigure 1: 12 lead ECG showing wide complex regular tachycardiaFigure 2:Two dimensional Echocardiography with apical four chamber view(A) with posterior tilt(B) showing a single solid mass arising from papillary muscle extending into left ventricular (LV) posterior wall upto crux of heart.LA-Left atrium,LV-left ventricleFigure 3: Two dimensional Echocardiography with subcostal long axis view showing a single solid mass arising from papillary muscle extending into left ventricular (LV) wall ,LA-Left Atrium,RA-Right AtriumFigure 4:Contrast Cardiac MRI showing well defined mass lesion arising from posterior wall of left ventricle extending posteriorly with exophytic component showing homogenous delayed enhancement(A),Size of the mass measuring 39x38mm(B)