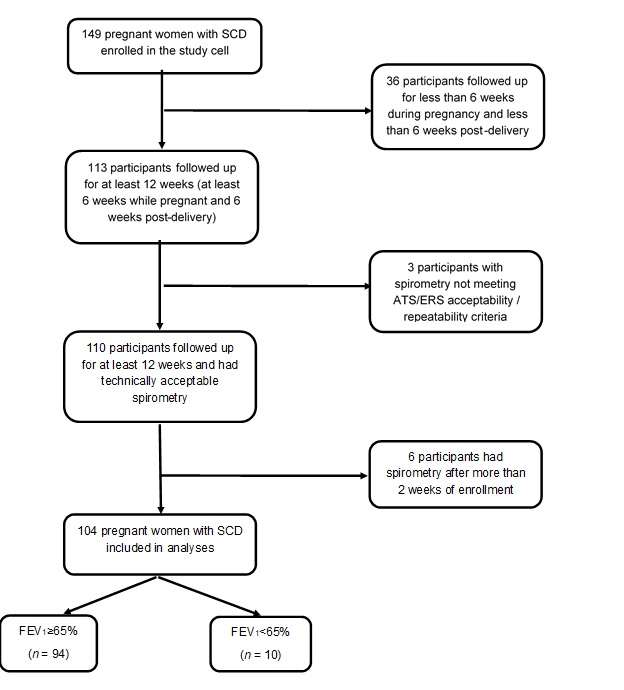
Objective: We tested the hypothesis that impaired maternal gestational pulmonary function, assessed by a moderate-to-severe reduction in FEV1% predicted, is associated with adverse perinatal outcomes in women with SCD. Design: Prospective cohort study. Setting: Tertiary referral centre Population: A total of 104 pregnancies in Ghanaian women with SCD aged 18–41 years. Methods: Participants were categorized into two groups (FEV1% predicted ≥ 65: n = 94; FEV1% predicted < 65: n = 10) based on spirometry performed before 28 weeks of pregnancy. The rates of adverse perinatal outcomes were compared between the two groups. Multivariable penalized logistic regression was used to estimate adjusted odds ratios. Main outcome measure: Fetal death, defined as fetus weighing>500g with no signs of life at birth. Results: Fetal death occurred more frequently in pregnant women with FEV1% predicated < 65 (30.0% versus 4.3%, p=0.02). FEV1% predicted < 65 was associated with a nearly 8-fold increased risk of fetal death (OR 7.81, 95%CI [1.59–38.38], p=0.01). Phenotype HbSS (3.41[0.68–17.19], p=0.13) and low maternal BMI (1.00 [0.84–1.20], p=0.96) were not associated with increased risk of fetal death. Conclusions: In pregnant women with SCD, low FEV1% predicted is associated with an increased risk of fetal death. Understanding the mechanism for low FEV1% predicted in pregnant women with SCD and improving gestational FEV1% predicted may result in a targeted intervention for decreasing fetal deaths. Keywords: Sickle cell disease, pulmonary function, FEV1, pregnancy outcomes, fetal death.