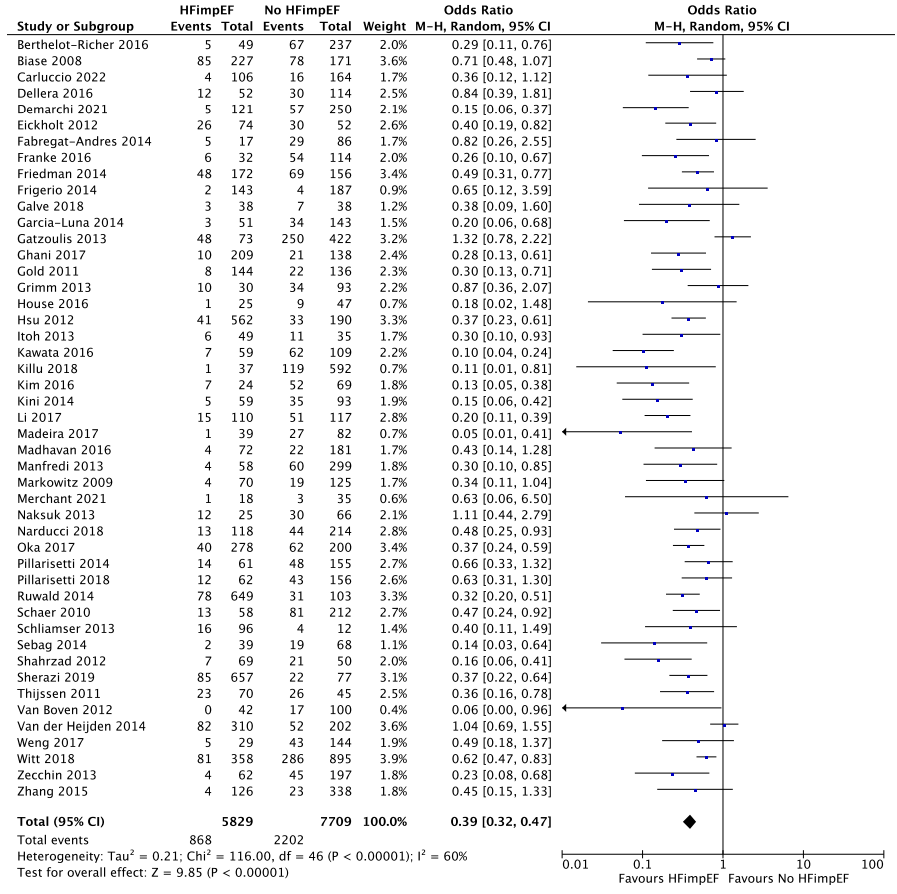
Background The benefit of implantable cardioverter defibrillator (ICD) therapy in patients who have heart failure with improved left ventricular ejection fraction (LVEF) to >35% after implantation (HFimpEF) is controversial. Methods Databases (Ovid MEDLINE, EMBASE, Web of Science, and Google Scholar) were queried for studies of ICD patients that reported the association between HFimpEF and arrhythmic events (AEs), defined as the combined incidence of ventricular arrhythmias, appropriate ICD intervention and sudden cardiac death (primary composite endpoint). Results A total of 41 studies and 38,572 patients (11,135 with HFimpEF, 27,437 with persistent EF <35%) were included; mean follow up was 43 months. HFimpEF was associated with decreased AEs (OR 0.39, 95% CI 0.32-0.47; annual rate (AR) 4.1% vs. 8%; P<0.01). Super-responders (EF >50%) had a lower risk of AEs than patients with more modest reverse remodeling (EF>35% and <50%, OR 0.25, 95% CI 0.14-0.46; AR 2.7% vs. 6.2%; P<0.01). HFimpEF patients who had an initial primary prevention indication had a lower risk of AEs (OR 0.43, 95% CI 0.3-0.61; AR 5.1% vs. 10.3%; P<0.01). Among primary prevention patients who had never received appropriate ICD therapy at the time of generator change, HFimpEF was associated with decreased subsequent AEs (OR 0.26, 95% CI 0.12-0.59; AR 1.6% vs. 4.8%; P<0.01). Conclusion HFimpEF is associated with reduced, but not eliminated, risk for AEs in patients with ICDs. The decision for replacing an ICD in lower risk subgroups should incorporate shared decision making based on risks for subsequent AEs and procedural complications.