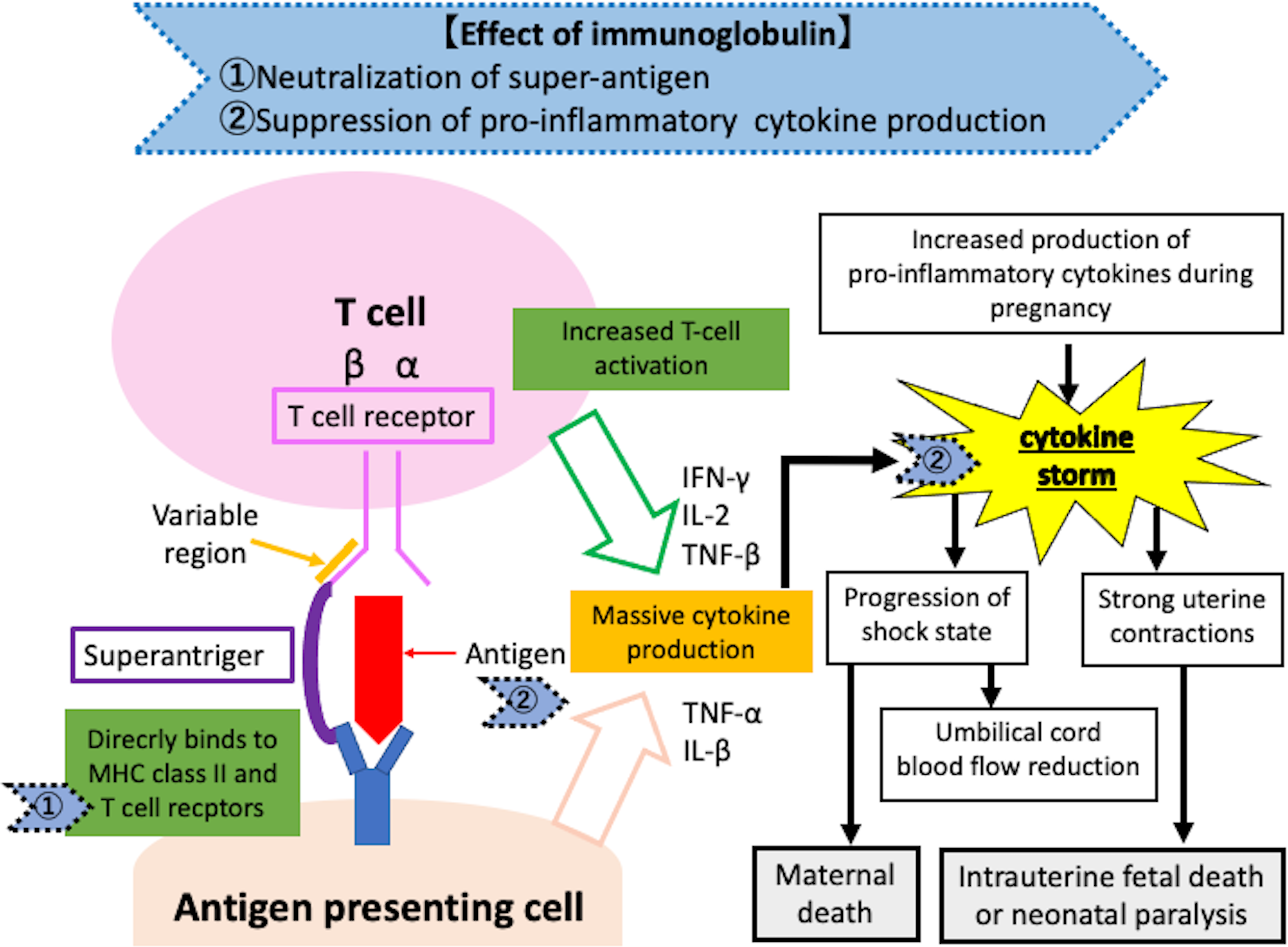
Fulminant streptococcal infection with early immunoglobulin introduction resulting in a favourable outcome for both mother and new-born: A case reportTakanori Sato, Rie Oyama, Tsukasa BABADepartment of Obstetrics and GynecologyIwate Medical University2-1-1 Ididori, Yaba-cho, Shiwa-gunIwateTel: 81-19-613-7111028-3695, JapanCo-author: Rie Oyama.E mail: [email protected] title: Successful treatment of STSS with immunoglobulinCase reportStreptococcal toxic shock syndrome (STSS) is Group A Streptococcus infection that causes rapidly progressive sepsis, disseminated intravascular coagulation (DIC), and multiple organ failure. STSS is the most common cause of sepsis-related maternal mortality1. Early diagnosis and intervention are important, but few reports on immunoglobulin as an adjunctive therapy. The cytokine production is elevated during pregnancy2, suppressing the cytokine storm is more important in sepsis caused by STSS in pregnant women than non-pregnant women, and anti-inflammatory immunoglobulin will likely be useful as an adjunctive therapy to improve maternal and infant prognosis. We report a case of STSS possibility treated using antimicrobial agents and immunoglobulin as adjuvant therapy. This patient of case report provided informed consent. We report a case of the potential of STSS treated with antibiotics and immunoglobulins as adjuvant therapy, and indicate the mechanism of effect of immunoglobulins on cytokine storm.A 37-year-old pregnant woman (gravid 5, para3) woman with a history of WPW syndrome and chronic thyroiditis. The patient had sore throat and fever of 39 °C on 32 +1 weeks, who was admministred in our hospital. At 32 + 4 weeks, her blood pressure and pulse were 79/48 mmHg and 140bpm, SpO2, 98% (oxygen mask, 6 L/min). Cardiotocography revealed delayed transient bradycardia, and we suspected septic shock and foetal insufficiency. Blood tests: WBC 14,740/μL, platelet 9.2 ×104/μL, C-reactive protein 11.1 mg/dL. Her qSOFA score: 1 (respiratory rate: >22 breaths/min), but her National Early Warning Score was 9 (respiratory rate, ≥25; oxygen demand, systolic blood pressure 101-110, heart rate ≥131/min), which is a warning value and corresponds to symptoms of sepsis due to STSS. Therefore, the antimicrobial agent was changed from cefepime to a combination of piperacillin and clindamycin, and an emergency caesarean section was performed 3 houre after admmited at our department. The baby was 2320 g, Apgar score, 1points/3 points (1 minute/5 minutes),umbilical artery blood pH 7.28. Obstetric DIC score was 3 points. Placental histopathology revealed stage 1 chorioamnionitis, but noGroup A streptococcal aggregation in the interchorionic space. On the second postoperative day, we were informed that Group A Streptococcus was detected in pharyngeal and blood cultures at the previous hospital, and antibacterial therapy with piperacillin and clindamycin for STSS and immunoglobulin were continued. Noradrenaline was also started as she had trouble maintaining her blood pressure on the first postoperative day, and dobutamine was added on the third postoperative day. On the fourth postoperative day, her respiratory condition worsened and bilateral diffuse frosted glass shadows were observed on chest radiography. Bilateral pleural effusions and pleural thickening were observed on computed tomography. Respiratory therapy with nasal high flow (NHF) was initiated. The patient was weaned from the NHF and switched to nasal cannula oxygenation on postoperative day 7. Oxygen administration was discontinued on postoperative day 15, and the patient was discharged on postoperative day 21 with improved bilateral diffuse frosted margins on chest radiographyDiscussionIn this case, STSS developed during pregnancy, but early delivery of the baby, antimicrobial therapy, and concomitant use of immunoglobulin from the early postoperative period onward resulted in a good outcome for both the mother and baby. In the field of obstetrics, perinatal STSS was described as “a condition that develops in pregnant women in the last trimester of pregnancy due to hematogenous myometrial infection mainly originating from the upper respiratory tract that induces labour pain and rapidly progresses to septic shock, resulting in a high rate of foetal and maternal death” in 20013,4. There is a trend toward poor prognosis for both the mother and new-born. In Japan, 24 (7.5%) of 317 maternal deaths were due to sepsis, and 13 (53.4%) were due to Group A Streptococcus infection between 2010 and 2016. A 2019 proposal by the Division of Medical Safety of the Japanese Society of Obstetricians and Gynaecologists stated that a modified Centor score should be used for pregnant women to facilitate early medical intervention and reduce maternal deaths due to STSS5. Penicillin and clindamycin are the basic antimicrobial agents of choice for STSS, and combinations containing clindamycin effectively suppress exotoxins and TNF-α and promote phagocytosis by inhibiting M-protein synthesis6,7. Meta-analysis reported that adjunctive immunoglobulin administration was associated with a significant reduction in mortality in STSS patients treated with clindamycin in 20188.The mechanisms of cytokine production and perinatal STSS are shown in Figure 1. Antigens are normally absorbed by antigen-presenting cells, fragmented into peptides, then recognised by T-cell receptors via the major histocompatibility complex (MHC) class II, which activates T cells. In contrast, superantigens bind directly to MHC class II and T-cell receptors without being taken up by antigen-presenting cells and produce numerous cytokines9,10, causing a marked inflammatory reaction via exotoxin11 and leading to septic shock. The production of cytokines such as TNF and IL-1β is also elevated during pregnancy due to changes in monocyte subsets13, and cases of perinatal STSS are prone to cytokine storms.Immunoglobulins exert effects similar to those of opsonin, along with phagocytosis-promoting, superantigen-neutralizing, anti-inflammatory, and antibody-dependent cytotoxic effects, and suppresses proinflammatory cytokine production11,13,14. Immunoglobulins have become a standard anti-inflammatory therapy for Kawasaki disease15. In this case, maintaining blood pressure became difficult on the first postoperative day, and noradrenaline was initiated along with immunoglobulin to suppress the cytokine storm caused by perinatal STSS. Procalcitonin levels were elevated the day after the culture results were obtained from the previous physician (postoperative day 3), but quickly decreased thereafter, and immunoglobulin was discontinued on postoperative day 4. Procalcitonin is produced by endotoxins and proinflammatory cytokines such as TNF-α, IL-1, and IL-6 in cases of severe bacterial infection16,17, and thus indirectly reflects the inflammatory state in the body. Procalcitonin may be an indicator of inflammation reflecting hypercytokinemia in cases of Kawasaki disease, and effectively predicts immunoglobulin refractoriness18. In this case, the reduction in procalcitonin levels following concomitant immunoglobulin use reflected STSS control and cytokine storm suppression, suggesting that the concomitant use of immunoglobulin may have been effective.In this study, we encountered a case of a mother and infant whose lives were saved by delivering the infant early, combined with the use of maternal antimicrobial therapy and combined immunoglobulin administration. The usefulness of combined immunoglobulin administration in perinatal STSS should be studied to further improve maternal and infant prognosis.