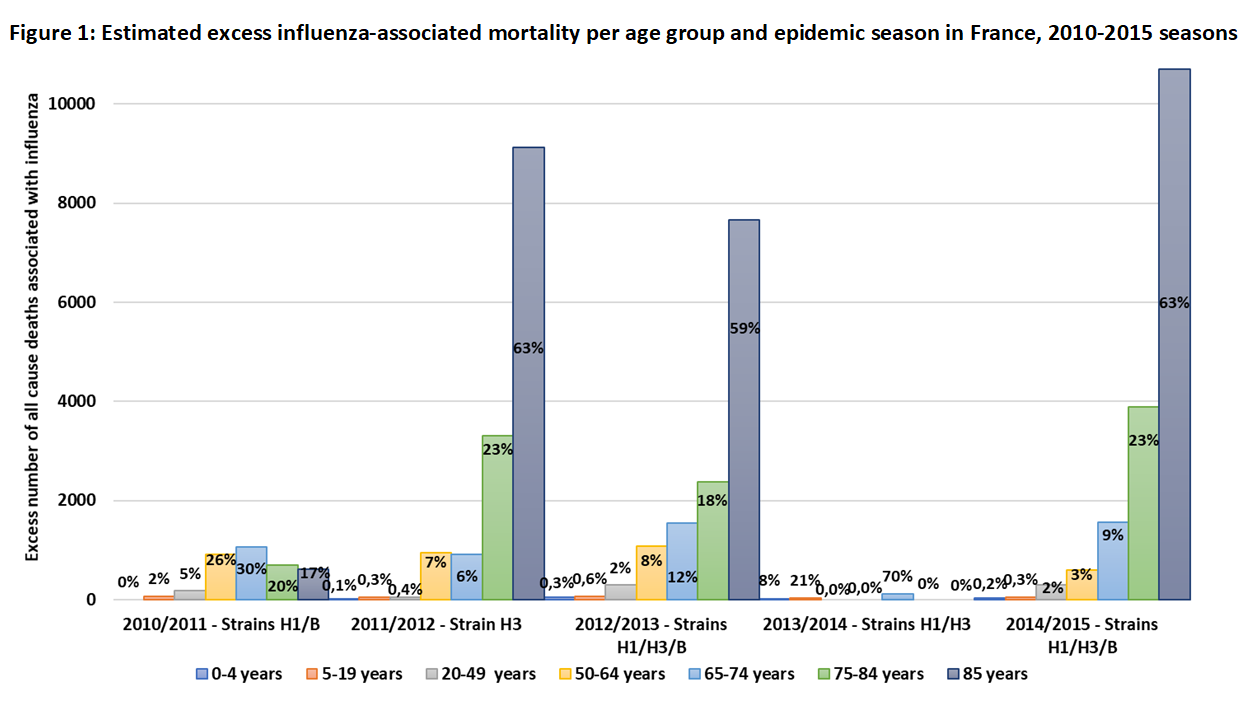
Background: In France, each year, influenza viruses are responsible for seasonal epidemics leading to 2-6 million cases. Influenza can cause severe disease that may lead to hospitalization or death. As severe disease may be due to the virus itself or to disease complications, estimating the burden of severe influenza is complex. The present study aimed at estimating the epidemiological and economic burden of severe influenza in France during eight consecutive influenza seasons (2010-2018). Methods: Influenza-related hospitalization and mortality data and patient characteristics were taken from the French hospital information database, PMSI. An ecological approach using cyclic regression models integrating the incidence of influenza syndrome from the Sentinelles Network supplemented the PMSI data analysis in estimating excess hospitalization and mortality (CépiDc – 2010-2015) and medical costs. Results: Each season, the average number of influenza-related hospitalizations was 18,979 (range: 8,627-44,024), with an average length of stay of 8 days. The average number of respiratory hospitalizations indirectly related with influenza (i.e., influenza-associated) was 31,490 (95% CI: 24,542-39,012), with an average cost of \euro141 million (range: 54-217); 70% of these hospitalizations and 77% of their costs concerned individuals ≥ 65 years of age (65+). More than 90% of excess mortality was in 65+ subjects. Conclusions: The combination of two complementary approaches allowed estimation of both influenza-related and associated hospitalizations and deaths and their burden in France, showing the substantial impact of complications. The present study highlighted the major public health burden of influenza and its severe complications, especially in 65+ subjects.