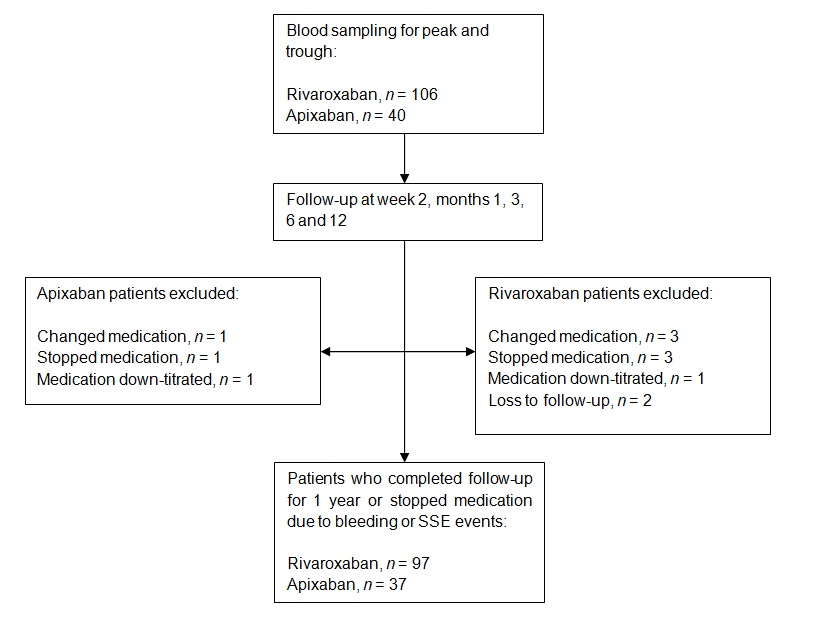
Aims: In a previous study, Singaporean Asians were found to have lower rivaroxaban plasma concentrations than Caucasians. This study attempts to identify predictors that may be associated with bleeding and stroke and systemic embolism (SSE) in Singaporean Asians taking rivaroxaban and apixaban. Methods: A total of 134 Singaporean patients on either rivaroxaban or apixaban for non-valvular atrial fibrillation were included for this study. Baseline characteristics were recorded at recruitment while bleeding and SSE events were recorded during a 1-year follow-up. Characteristics of patients with or without bleeds were compared using relevant statistical tests. Multivariable regression that included covariates with p < 0.1 from an initial univariable regression was performed to analyze predictors that resulted in higher risk of bleeding in patients. Results: Median creatinine clearance (CrCl) was significantly lower in patients on rivaroxaban who experienced bleeds as compared to patients who did not experience bleeds (61.5 vs 70.8 mL/min, p = 0.047), while concomitant simvastatin use was found to be independently associated with a six-fold increased risk of bleeding [Adjusted OR = 6.14 (95% CI: 1.18 – 31.97), p = 0.031] for rivaroxaban after controlling for body mass index, CrCl and having experienced a previous SSE. Conclusion: Our findings suggest that concomitant use of simvastatin with rivaroxaban may be associated with bleeding events in an Asian cohort. Further studies using physiologically-based pharmacokinetic modeling are required to investigate the drug-drug interactions between these drugs. Keywords: Atrial Fibrillation, Bleeding, Rivaroxaban, Simvastatin